
Protocols
Airway Management and General Difficulty Breathing
Airway Management and General Breathing Difficulty
Establish and maintain open airway. No matter what the condition, the airway must remain patent at all times.
Head Tilt-Chin-Lift or Jaw Thrust Head Tilt Maneuver: No neck injury suspected. Head Tilt-Chin-Lift is temporary and must be replaced with an upper airway adjunct unless the patient begins adequate spontaneous ventilations. Indications: Any unresponsive patient without history of MOI. Cardiac arrest without MOI. Apneic patients without MOI.
Jaw Thrust In-line Maneuver: Used with suspicion of spinal injury. Use of a Jaw Thrust is temporary and must be replaced with an upper airway adjunct unless the patient begins adequate spontaneous ventilations. Indications: Unresponsive trauma patient. Unresponsive patient with an undetermined MOI.
Note: If difficult to ventilate or air will not enter always reposition the head and attempt ventilation again.
Suction secretions as needed.
Patient needs suctioned immediately when gurgling sound is heard with artificial ventilations. Suction devices may not be able to remove large obstructing particles in the airway. Roll patient to the side and remove manually large obstructions then follow with mechanical suctioning if needed.
If patient produces frothy secretions as rapidly as suctioning can remove, suction for 15 seconds, artificially ventilate for 2 minutes, and continue in that manner. Consult medical direction for this situation.
Assess quality, rhythm and rate of ventilations. Note: Mental status and/or cyanosis is not always a main determining factor to indicate need for oxygen. Look at rate, rhythm and quality to decide on the best oxygen device.
Signs of inadequate ventilator status (if patient is breathing). Adult: Rate less than 12 or greater than 20/minute. Rhythm irregular, such as taking a series of deep breaths followed by periods of apnea. Quality of auscultated breath sounds diminished, noisy or absent. Reduced flow of expired air out the nose and mouth. Chest expansion unequal or inadequate results in reduced tidal volume and minute volume. Increase effort to breathing using accessory muscles. Skin may become pale or cyanotic and cool and clammy with or without agonal respirations.
Techniques of artificial ventilation if needed.
The following patients need artificial ventilations: Any patient with reduces minute volume (breathing rate and depth). Respiratory arrest will require approximately 12 ventilations per minute. Reduces tidal volume and a rapid rate (hyperventilation) will need rate control. Reduced minute volume (hypoventilation) require rate and volume assistance.
- Hyperventilating not associated to hyperventilation syndrome (panic attack) patient: Explain procedure to responsive patient. Place mask over nose and mouth. Initially assist ventilate at the rate at which patient has been breathing. Over the next 5-10 breaths, slowly adjust the rate and deliver tidal volume until adequate minute volume.
- Hypoventilating patient: Place mask over nose and mouth. Initially assist ventilate at the rate at which patient has been breathing. Over the next 5-10 breaths, slowly adjust the rate and deliver tidal volume until adequate minute volume.
Special situations:
- Laryngectomies (stomas): Check for obstructions and suction. Upon artificial ventilations air escapes from mouth and nose, close the mouth and nostrils.
- Infants and children: Do not hyperextend the head. Do not use pop-off valve on BVM for infants/children.
- Dental appliances: Dentures should be left in place. Partial dentures may become dislodged. Leave in place, but be prepared to remove dentures if they become dislodged.
Equipment for artificial ventilations.
2 person BVM. Advantages good seal and two hands squeezing the bag. Disadvantage requires two rescuers.
1 person BVM. Advantage only one rescuer needed. Disadvantage requires a skilled rescuer. Only the highly skilled and frequent users are able to obtain and maintain an adequate mask to face seal.Flow Restrictive Ventilator
Flow restrictive, oxygen-powered ventilation device. Major advantages provides high concentration of O2 while allowing EMT to use 2 hands to maintain seal. Major disadvantage may not be used with all types of patients for example lung disease and children.
Mouth to mask with one way valve. Advantages one rescuer device.
Equipment for supplemental oxygen delivery.
Non-rebreather mask: Oxygen rate 10 to 15 liters. Do not go under 10 LPM with a non-rebreather mask.
Nasal cannula: Rarely the best method of delivering adequate oxygen to the hypoxic patient. Should only be used when patient will not tolerate a non-rebreather mask, despite coaching from healthcare professional.
Artificially ventilate versus Supplemental Non-Rebreather mask.
If initial assessment reveals respiratory distress as listed under number 3 then proceed to the following:
- PulseOx low
- ETCO2 high
- Tidal volume low
- Rate too low or high
If patient is responsive and the breathing is adequate (good rate, quality and volume) oxygen still may be indicated.
- PulseOx 94 to 100 = Room Air
- PulseOx 90 to 94 = NC 1-4 LPM
- PulseOx less than 90
❖ Good Tidal Volume NR 10-12 LPM
❖ Poor Tidal Volume BVM 15 LPM
If patient is responsive and the breathing is inadequate (poor rate, quality or volume) and assist the patient’s ventilation using methods listed in number 4.
If the patient is unresponsive and the breathing is adequate (good rate, quality and volume), provide high concentration oxygen non-rebreather.
If the patient is unresponsive and the breathing is inadequate (poor rate, quality or volume) use methods listed in number 4.
Defining mild, moderate and severe breathing difficulty.
- Mild (dyspnea): May be hypoxic but can move an adequate tidal volume. Can answer questions in sentences and alert. Administer non-rebreather. Start to treat underlying causes.
- Moderate (Mild Failure): May be hypoxic but can move an adequate tidal volume. Having difficulty answering questions. Wheezing can be a upper and lower whistling sound. Still awake but may be restless/irritable. May not let you assist breathing with BVM at this time. Administer non-rebreather mask. Get ready with BVM if needed. Start to treat underlying causes.
- Severe (Moderate/Severe Failure): Respiratory Failure is clearly present. Getting sleepy. Not speaking or speaking very few words. Patient usually sitting upright (tripod). BVM and timed with inhalation.
IF PATIENT BENEFIT FROM BRONCHODILATOR AND THE CLINICAL SIGNS INDICATE POSSIBLE BENEFIT FROM ITS USE:
CONSULT MEDICAL CONTROL ALWAYS FIRST.
- EMT – If patient has prescribed bronchodilator may be indicated to assist patient in delivery.
❖ Contraindications: Inability of patient to use device. Inhaler not prescribed for the patient. No permission from medical direction. Patient already met maximum dose.
- Paramedic
❖ albuterol 2.5mg/3mL Neb repeat once in 10 min or 90mcg x 2 MDI
❖ Atrovent 0.5mg/2.5mL Neb (Good for questionable heart condition)
❖ Xopenex 1.25mg/2.5mL Neb
❖ terbutaline 0.25mg SubQ
❖ Severe cases: May mix albuterol with Atrovent.
Insert airway Adjuncts if needed.
Nasopharyngeal airway: Less likely to stimulate vomiting. Measure nose to ear, lubricate with water-base, bevel to the septum. Examples of patient needing nasal airway: Unresponsive and snoring or unresponsive with gag reflex.
Oropharyngeal airway: Unresponsive patient without gag reflex. Measure from corner of mouth to ear or angle of the jaw. Adult rotate 90 to 180 degrees, pediatric depress tongue and place or rotate up to 90 degrees. Examples of patient needing oral airway: Unresponsive, apneic patients. Any apneic patient being ventilated with a BVM.
Benefit of OPA:
- Evaluate gag to assess if airway is protected.
- Keeps teeth apart for BVM
- Allows assessment for how wide mouth can be opened for intubation.
- Aids in suction of lower airway.
Transport in POC.
Perform ongoing assessment every 5 minutes
If patients ventilatory drive is failing, prolonged BVM or patient cannot protect airway consider advanced airway.
LMA – EMT & Medic skill
King Tube – EMT & Medic skill
CombiTube – EMT & Medic skill
- Contraindicated with esophageal varices
ETT Intubation – Medic Skill
If spontaneously breathing consider
- Nasal intubation with whistle tip to bypass gag.
- Conscious sedation intubation
❖ Ketamine 1-2mg/kg
❖ Propofol 2mg/kg
❖ Etomidate 0.3mg/kg
❖ Midazolam 1mg SIVP
❖ Then give a little narcotic – Fentanyl or Morphine
❖ Most common is Versed and Fentanyl
- Rapid sequence intubation (RSI) Watch Video: RSI
❖ Sedative
➤ Ketamine 1-2mg/kg
➤ Propofol 2mg/kg
➤ Etomidate 0.3mg/kg
➤ Midazolam 1mg SIVP
❖ Neuromuscular Blocker
➤ Vocuronium (ROC) 1mg/kg Adult – 100mg (Give before sedative)
➤ Succinylcholine 1mg/kg Adult 100mg (Give after sedative)
If positive pressure is needed in the lungs consider ETT (PEEP)
Cardiac Monitor and AED
Cardiac Monitor and AED Manual Cardiac Monitor:
- Defibrillation: Watch Defib Video
- Unconscious patient: Perform quick look to identify if V-Fib or V-Tach pulseless is present.
- Deliver 360J or biphasic energy range.
- Perform 2 minutes of immediate CPR.
- If patient is down for more than 4 to 5 minutes perform 2 minutes of CPR prior to defibrillation.
- Paddle / Hands Free Pads
AED Machine:
- AED PADS size: 0 to 8 years old use pedi pads provided with AED.
- If no pedi pads are available may use adult pads.
- Adults AED pads are for age 8 and above.
Manual Cardiac Monitor:
- Pedi paddle/pads are used on 10 kg (1 year old) and less.
- Studies show that hands-free provides quicker time to shock that paddles.
Note:
- If AED is analyzing let it perform as needed. Let AED deliver the first shock if needed. Then remove AED and place patient on manual cardiac monitor.
- Semi automated defibrillator is the same as an AED learned in EMS school. Semi just means the EMT has to at lease press one button.
- Primary shockable rhythms are Ventricular Fibrillation and Pulseless Ventricular Tachycardia.
- Prepare the patient for transport after no shock advised, or after patient regains pulse.
- If pulse is present then check breathing. If breathing or not refer to General Breathing Difficulty Protocol
- If AED is used keep it attached until ALS arrives then use manual cardiac monitor.
Pad/Paddle placement
- Place pads 1 to 2 inches away from implanted devices.
- Shave if needed.
- Remove medication patches.
- Chest must be dry.
- Avoid direct contact with metal.
Place pads/electrodes as advised.
- Most common placement: Pad 1 right of sternum below clavicle or breast. Pad 2 place 2 inches below left armpit.
- Anterior Posterior position: Left infrascapular under scapula other Left infraclavicular.
- Left and Right infrascapular
- Anterior Apex Left intrascapular
Synchronized Cardioversion: Watch Synch Video
- Patient is extremely rapid heart rate and cardiac in origin.
❖ Synch avoids R on T. Delivers electricity on QRS not the T wave.
❖ Use paddles/pads as stated above.
❖ 100J, 200J, 300J, 360J monophasic or equivalent biphasic energy.
➤ Check for pulse between each shock.
➤ In emergency titrate sedative for pain. Do not pre-load.
Transcutanious Pacing: Watch Pacing Video
- Used on bradycardic unstable patients.
❖ Pad selection as stated above.
❖ Unstable patient set rate to 80 beats per minute – set milliamps (mA) to 80. If no capture increase mA.
If capture present at 80 reduce and titrate.
❖ In emergency titrate sedative for pain. Do not pre-load.
Allergic Reaction
Allergic Reaction Signs and symptoms:
- Mild reaction normal vitals with urticaria (hives), itching.Urticaria
- Moderate reaction is mild reaction plus respiratory compromise.
- Severe reaction (anaphylaxis) has mild and moderate and now circulatory collapse.
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
❖ Never underestimate the severity of an allergic reaction. If breathing is adequate but likely to deteriorate rapidly, place patient on a non-rebreather at minimum care. Even if patient is only showing signs of a mild reaction. Due to potential of rapid deterioration be proactive, place on oxygen.
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Establish IV Large Bore
- Ensure scene is safe from bees, wasps, etc… Move patient to safety.
- Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor Protocol and/or CPR Chart Protocol.
- If breathing difficulty is present go to General Difficulty Breathing Protocol to maintain airway if needed then return to this protocol.
Care:
- If Mild (Localized Reaction) only:
❖ Benadryl 25mg-50mg IM or IV.
❖ Pedi: Benadryl 1mg/kg IV or IM.
- If Moderate Dyspnea, but SBP > 90mmHg without Shock, Hypoperfusion, or Critical Airway:
❖ Bronchdilate
➤ albuterol 2.5mg/3mL Neb repeat once in 10 min or 90mcg x 2 MDI.
➤ Atrovent 0.5mg/2.5mL Neb (Good for questionable heart condition).
➤ Xopenex 1.25mg/2.5mL Neb
➤ terbutaline 0.25mg SubQ
➤ Severe cases: May mix albuterol with Atrovent.
➤ Epi 1:1,000
✔ EMT: EPI-PEN 0.15mg (pedi) or 0.3mg (adult) IM
✔ Paramedic: 0.3-0.5mg SubQ
❖ Antihistamine
➤ Benadryl as listed in mild reaction.
❖ Steroids
➤ Dexamethasone 4-24 mg IV
➤ Solu-Medrol 60-250 mg IV.
✔ Pedi dose: Solu-Medrol 1-2mg/kg IV, Dexamethasone 0.25mg/kg IV.
- If Severe (Shock), Severe Hypoperfusion, Critical Airway or SBP < 90mmHg:
Supine position with legs elevated or trendelenburg position, if tolerated.
EPI
- EMT: EPI_PEN as described in moderate reaction.
- Paramedic Epi 1:10,000 0.3mg-0.5mg IV or 0.5mg 1:1000 sublingual injection: administer as soon as possible. Do not delay epinephrine sublingual injection administration while attempting IV access. Pedi dose: 0.01 to 0.1mg/kg IV 1:10,000.
Benadryl as stated in mild reaction.
250-1,000 ml fluid boluses and frequent reevaluation (may require 2 Liters)*. Pedi bolus: 20mL/kg x 3.
Steroids as described in moderate reaction.
Expedite transport
Perform an ongoing assessment every 5 minute
Paramedic: Prepare for need of intubation or surgical airway.
Seizure
Seizures
- If patient is actively seizing protect from the environment. Avoid physical restraint if possible.
- Only treatment possible while seizing is try treating the cause of the seizure:
examples:
❖ If diabetic seizing treat diabetes.
❖ If hyperthermia treat temperature.
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- Establish IV
Actively Seizing:
- 2 to 5mg valium IV slow or IM until seizure stops or max dose 10mg. Double dose if rectal.
❖ Pedi 0.1-0.5mg/kg
- 1 to 5mg Versed IV slow or IM.
❖ Pedi 0.1mg/kg
- 4mg Ativan IV slow. Not recommended for IM.
- Narcan 2-4mg IV or IM if seizure is of narcotic causes (rare).
❖ Pedi 0.1mg/kg
Hypoglycemic Seizures: (adult <60mg/dL – pedi <40mg/dl):
- D50 25-50g IV
❖ Pedi 1g/kg D25% or D10%
- If no IV Glucose Gel 25-50g Oral Mucus or Rectal
- If no IV Glucagon 1mg IM
- Note: If seizure actively stops after Glucose/Glucagon for diabetic seizures do not give Valium.
Once muscle convulsions have stopped:
- Evaluate responsive, airway, breathing, circulation.
❖ If pulseless and apneic go toAED/Cardiac Monitor protocol and/or CPR Chart Protocol.
❖ If breathing difficulty if present go to General SOB protocol to maintain airway if needed then return to this protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma suspected protect head and spine.
- If low BP place supine.
If febrile seizure
- Cool with tepid water.
- Pedi: Consider 15mg/kg rectal liquid Tylenol.
Note: Most common adult seizure reason is not taking anti-seizure medication. Transport
- If first time seizure
- Other underlining medical problem present
- If history of past seizures and not responding as expected like previous seizures transport.
Perform ongoing assessment every 5 minutes
Altered Medical Status - Diabetes
Altered Mental Status – Diabetic Emergency Signs and symptoms:
- Rapid onset of confusion. Unusual exercise. Staggered gate. Hunger. Seizure activity. Anxiousness, combative, or restlessness. Tachycardia. History of diabetes. Blood glucose of < 60 mg/dl (Pedi: <40mg/dl).
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- Establish IV
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If convulsions are present refer to Seizure protocol.
- If trauma suspected immobilize the patient and refer to Trauma protocols.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
Hypoglycemic: Glucose <60mg/dL (Pedi <40mg/dl)
- Sugar foods and drinks
❖ If conscious and alert, not nauseated or vomiting and can follow directions may give; water with sugar, fruit juices, soft candy (simple sugars).
- Glucose
❖ D50% 25-50g IV. (Pedi: 1g/kg D25% or D10%)
❖ Oral Glucose Gel 25-50g Oral mucus or rectal (Pedi 1g/kg)
- Narcan 2mg-4mg IV if no improvement with D50% (Pedi: 0.1mg/kg)
- Glucagon 1mg IM if no IV and unresponsive.
Non-Hypoglycemic: Glucose >80mg/dL
- Narcan 2-4mg IV, IM.
Note:
- Recent head injury contact medical control to see if relative contraindication at this time.
- If BS low and Glucose or Glucagon administration works do not give Narcan.
- If Glucose, Glucagon and Narcan do not work consider other causes of AMS
Transport Ongoing assessment every 5 minutes
Myocardial Infarction
Cardiac Compromise and Acute Coronary Syndromes Signs and Symptoms:
Chest pain/discomfort. Radiating pain to arms, neck, back. Sudden onset of sweating. Difficulty breathing. Cool, pale skin. Light headed, Anxiety or irritability. Feeling of doom. Abnormal or irregular pulse rate. Abnormal blood pressure. Nausea and/or vomiting.
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- Establish IV
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
- If pulmonary edema is present or possible use caution when lowering the head and evaluate breath sounds often.
Adult Care:
- Aspirin 160-325mg PO (chew and swallow).
❖ EMT may concider ASA with medical control permission.
- Obtain 12 lead ECG within 5 minutes of arrival.
❖ If Inferior Infarction (Leads II, III, aVF).
➤ Perform right sided 12 lead or 15 lead to role out inferioposterior MI.
✔ 15 lead (r/o posterior involvement)
▪️ Lead V4R: 5th IC space midclavicular on right side
▪️ V8: 5th IC space midscapular line
▪️ V9 goes between V8 and the spine
▪️ Place Lead V5 wire on V8 and V6 wire on V9. Attach V4 wire to the V4R position
✔ Confirm RV Failure is not present before Nitro/Morphine.
- If BP <90mmHg
❖ give 250mL fluid bolus IV if no pulmonary edema is present, titrate BP to >90mmHg.
- If BP >90mmHg
❖ Nitroglycerin SL 0.4mg up to 3 doses every 5 minutes.
➤ EMT: If patient has prescription contact medical control prior to assisting.
❖ If pain continues after nitro give:
➤ Morphine 2-4 mg increments to max 10mg IV-Slow. (Best drug)
➤ Fentanyl 50mcg IV Slow (Does not lower BP like Morphine)
➤ Nitrous Oxide self administered. (Good for pain with low BP)
➤ If N/V develops
✔ Phenergan 6 to 12mg IV Slow push
✔ Zofran 2-4 mg IV
- If BP extremely low consider vasopressors Dopamine or Levophed for cardiogenic shock.
Note:
- Contraindications Nitro and Morphine: Absolute contraindication if BP less than 90mmHg.
- Recently taken Viagra, Silderafil, Cialis, Tadalafil, Levitra, or Vardenafil within 24 hours do not administer Nitroglycerin unless advised by contact medical control.
- Nitroglycerine may take up to 2-3 minutes for full action. This is why you wait 2-3 minutes then take BP before you decide on another dose.
Record time and vitals
- 2-3 minutes after each drug given.
Do not unnecessarily delay transport.
- Keep patient calm.
Clot buster medication goal time is within 1 hour of onset of symptoms Ongoing assessment every 5 minutes
Stroke
Altered Speech, sensory, motor function – STROKE Emergency Signs and symptoms:
Cincinnati Stroke Scale: Arm drift, speech, facial droop. Confusion, poor balance, intoxicated appearance.
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Take BP in both Arms.
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- Establish IV
- 12 Lead
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
Patient positioning.
- If conscious and alert place in POC. Preferably semi-fowlers position.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
Speak to the patient and explain all procedures.
- Many times they may appear unresponsive but can hear your words.
Contact receiving hospital early to meet 3 hour window for clot busters. Avoid unnecessary oral glucose and nitro if a stroke is suspected.
- If hypoglycemic go to Diabetic protocol.
Perform ongoing assessment every 5 minutes. Blood Pressure
- Do not treat BP unless over 220/110.
❖ Labetalol 10mg IV
Note: If low BP present consider another cause for AMS.
Behavioral Emergency
Behavioral Emergency Ensure your safety and prepare for possible violence.
- Always have a partner.
- Do not rush the call.
- Keep your back to the exit.
- Call for law enforcement if needed for safety.
- Look at surroundings when you enter.
- Look at patient body language.
- It is not abandonment to leave an unsafe scene if patient contact has already been established.
Role Out Other Causes for AMS Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing protocol
- Test glucose
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If blood sugar low go to Diabetes protocol.
- If poison or drug overdose go to Poison protocol or Drug/ETOH protocol and then return to this protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
- Avoid letting the patient walk to ambulance. Elopement risk.
Assess patient for possible self inflicted injury. Patients are good at hiding injuries. Establish and maintain in-line spinal if suspected injury from hanging or trauma If patient is responding keep them calm.
- Do not rush.
- Do not give into their hallucinations.
- Get their psychiatrist staff or family member on the phone or to the scene.
If patient become violent and threatens physical harm to self or others restrain.
- May not restrain verbal abuse only physical.
Ongoing assessment every 5 unstable every 15 stable Do not leave patient alone Suicide risk.
- Any person can commit suicide.
- Look for the person with the means and the plan.
- Do they have a gun, or drugs to overdose on, or a plan.
May restrain if physical danger to self or others
- Use soft restraints 4 point
- Tie to bed not handrail
- Monitor ECG
- Pulse-Ox
- Document airway and PMS in restrained extremities every 5 minutes.
If needed Haldol may be given to calm patients
- Contact medical control for dosing.
Transport
- Do not allow them to walk to ambulance. Insist they are placed on the stretcher with all safety straps secure.
- Allow them to bring any personal item if they feel more comfortable.
- Listen to them. This is mental not physical. If they are not talking you cannot figure out how to help them.
Refusal:
- May not refuse even if A&Ox4 if you think they will carry out a plan of suicide.
- With medical control permission you may leave them with a family member. But only with medical control permission.
Recognize signs of stress for EMS workers
- Lack of sleep, drinking alcohol, lack of sex, depression, guilt, drugs.
- If an EMS worker shows signs they should be directed to a stress management course. Look out for each other.
Heat Emergencies
Heat Emergencies Remove from hot environment and/or humidity. Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- IV x 2 Large Bore
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If seizure go to Seizure protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
Turn up air conditioner to maximum. Remove excessive clothing. Heat Exhaustion or Heat Cramps: If skin is cool, moist, and pale (heat exhaustions) cool patient with wet compresses, fan, place supine raise feet. If not N/V give water by mouth 1-2 glass every 15 minutes. Monitor ECG, D-stick, IV fluid 500mL over 15 minutes. Heat Stroke: If skin is hot and dry (above 104 degrees) or even moist (heat stroke) pour water over patient, place cold packs in armpit, groin, fan patient. Tap a fire hydrant and soak patient. Just get the temperature out of the danger zone by any means possible. Key for heat stroke vs heat exhaustion is low BP.
- When pt starts to shiver slow the cooling process. IV fluid 500mL bolus x 3 does not acutely overload hydrate.
- Prepare for possible seizure activity. Go to Seizure protocol.
Transport Perform assessment every 5 minutes.
Hypothermia - Generalized
Generalized Cold Emergency – Hypothermia
Note: Never give up until they are warm, and dry. Only then are they dead.
Remove from cold environment. Prevent further heat loss.
Evaluate responsive, airway, breathing, circulation.
Standard Care/Monitoring:
- Pulse check should last a minimum of 30 seconds to 60 seconds before starting CPR.
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- IV
Protocols
- If you suspect localized cold emergency (frost nip/bite) with no general hypothermia go to Cold Injury protocol.
- If pulseless and apneic go to AED/Cardiac Monitor protocol
❖ If severely hypothermic deliver only one shock for V-Fib and perform CPR.
❖ Contact medical control for further orders.
- If severely hypothermic contact medical control prior to administering any drugs.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
❖ Warm and humidify the oxygen being delivered.
❖ Warm/hot packs not on body but within the blankets.
❖ Warm IV bags to 96-104 degrees.
Patient positioning.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
- Avoid rough handling and do not allow to walk around.
- Keep them flat. Tilting patient may lead to cardiac arrest V-Fib.
Remove all wet clothing, jewelry, etc…
If patient is alert and not confused begin to actively rewarm. Examples: Drink warm liquid not caffeine or alcohol.
Do not allow to eat or drink stimulants. Caffeine and alcohol are most common not to allow.
Do not rub.
Have AED/Cardiac monitor ready for V-Fib.
- If severely hypothermic only provide one 360J shock in V-fib until body temperate rises.
- Also withhold drug therapy until body temperature rises. Check with medical control prior to additional electric therapy and drug therapy.
Transport horizontal position. Backboard may be needed.
Perform ongoing assessment every 5 minutes.
Localized Cold Injury
Local Cold Injuries – Frost Nip and Frost Bite
Remove patient from the cold environment. Frost bite toe 2Frostbite toe
Standard Care/Monitoring:
- Pulse check should last a minimum of 30 seconds to 60 seconds before starting CPR.
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- IV
- If you suspect generalized cold emergency go to Hypothermia protocol.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
- Note: Avoid rough handling and do not allow to walk around.
Remove all wet clothing, jewelry, etc…
Cover affected frost nip/bite skin with dry sterile dressings.
If early; Frost Nip:
- Immobilize affected extremity, do not rub, do not re-expose to cold.
If late; Frost Bite:
- Do not rub, do not break blisters.
- Do not apply heat to rewarm.
- Do not allow them to walk on extremities.
- Try to separate fingers and toes unless already frozen together.
If required / instructed by medical control to rewarm:
- Immerse tissue in 104 degree water.
- Keep water at constant temperature.
- Keep immersed until color and feeling return to normal.
- Dress wound and protect from refreezing.
- Pain management
❖ Morphine 2-10 mg IV
❖ Fentanyl 50 to 200 mcg IV, IN
Transport
- Advise receiving facility to allow for equipment set up in ED.
Poisoning
Poisoning Emergencies
Protect yourself.
Evaluate responsive, airway, breathing, circulation.
If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
If allergic reaction go to Allergic Reaction protocol.
If seizure go to Seizure protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma protect head and spine.
- If low BP place supine.
Contact medical control and/or poison center for directions with treatment.
Ingested: IF PATIENT NEEDS ACTIVATED CHARCOAL AND THE CLINICAL SIGNS INDICATE POSSIBLE BENEFIT FROM ITS USE:
ALWAYS CONSULT MEDICAL CONTROL FIRST.
Facilitate administration of activated charcoal.
Indications (meets all of the following): Exhibits signs and symptoms of ingestion overdose/poisoning emergency. Specific authority by medical direction.
Dose: Activated charcoal 1g/kg or about 30-100g for adults and 12.5 to 25g for children.
Contraindications:
- Nauseated prior to administration.
- Ingestion consumed over 1 hour ago.
- Cannot swallow or follow instructions.
- Do not administer in acid or alkali poisoning.
- Avoid alcohol, kerosene, gasoline, metal poisoning because charcoal will not bind.
- No permission from medical direction.
- Patient already met maximum dose.
Side effects: Black stool, nausea /vomiting.
Note: Syrup of Ipecac is usually not given to ingestion overdoses/poisonings in EMS. Must be given within 20 to 30 minutes of ingestion. If patient becomes unresponsive will still vomit leading to an airway concern. Dose: 30mL in 8 oz glass of water.
Inhales:Remove from environment. High concentration of oxygen. Go to General Difficult Breathing protocol.
Injected: Scrape stinger from site. Wash injection site with soap and water. Watch for allergic reaction. Go to Allergic Reaction protocol.
Absorbed: Brush off dry chemicals, remove clothing and flush for at least 20 minutes.
If organophosphate poisoning.
Signs and symptoms of SLUDGE – Salivation, Lacrimation, Urination, Defecation, GI irritability, Eyes constrict.
Poisoning will stimulate parasympathetic stimuli.
Pesticides, fertilizers cause organophosphate poisonings. Think Nerve Gas.
Most commonly absorbed through skin. Irrigate skin.
Atropine is drug of choice – 2 to 5 mg loading dose may repeat.
EMT should consider ALS back-up on all overdoses/poisoning if unstable.
Potential for seizures. Go to Seizure protocol.
Transport.
Perform ongoing assessment every 5 minutes.
Drug or Alcohol Emergency
Drug or Alcohol Emergency
- Protect yourself from violent patients. Keep your back to the exit. Never be alone.
- Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine and elevate legs.
Contact medical control and/or poison center for directions with treatment.
Ingested pills/solids: IF PATIENT NEEDS ACTIVATED CHARCOAL AND THE CLINICAL SIGNS INDICATE POSSIBLEBENEFIT FROM ITS USE:
ALWAYS CONSULT MEDICAL CONTROL FIRST.
Facilitate administration of activated charcoal.
Indications (meets all of the following): Exhibits signs and symptoms of ingestion overdose/poisoning emergency. Specific authority by medical direction.
Dose: Activated charcoal 1g/kg or about 30-100g for adults and 12.5 to 25g for children.
Contraindications: Nauseated prior to administration, cannot swallow or follow instructions. Do not administer in acid or alkali poisoning. Avoid alcohol, kerosene, gasoline, metal poisoning because charcoal will not bind. No permission from medical direction. Patient already met maximum dose.
Side effects: Black stool, nausea /vomiting.
For additional treatment options go to Poisoning protocol.
Potential for seizures. Especially with DT withdrawals. Go to Seizure protocol.
Transport.
Perform ongoing assessment every 5 minutes.
Acute Abdominal Pain
Acute Abdominal Pain Signs and symptoms: Nausea / vomiting, diarrhea, cramping, vomiting blood, tachycardia (bleeding), rebound tenderness (spillage). Any complaint in the abdominal area should be evaluated by a doctor.
Evaluate responsive, airway, breathing, circulation.
If pulseless and apneic go to AED protocol and/or CPR Chart protocol.
If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
If bleed go to Hemorrhage and Shock protocol.
If OB/GYN go to Pre-delivery protocol.
Patient positioning.
- If conscious and alert place in POC, usually with knees flexed.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
Evaluate for shock internal bleeding. Go to Bleeding / Shock protocol.
PASG may be indicated for abdominal and pelvis bleeding to provide direct pressure and shock. Go to Bleeding / Shock protocol
Do not delay transport to diagnose abdominal complaints. Too difficult and not very accurate in EMS.
Reassess every 5 minutes.
Avoid narcotic pain medication until diagnosed or medical control permission.
- Kidney Stone – flank pain to groin, blood in urine.
- Gallbladder – RUQ radiating to right shoulder. 5 “f”-er
- Liver – URQ dull pain with fever, night sweats.
- Peptic Ulser – May feel better after diluting acid.
- Pancreatitis – May not feel better after eating.
- Appendicitis – RLQ to navel.
- Diverticulitis – LLQ pain and distention.
Submersion and Drowning
Submersion/Drowning
Safety first. If not trained, or do not have correct equipment (personal floatation devise – PFD) or cannot make the scene safe do not enter water. How to get out of water: Reach, throw, row and final go if you have the safety equipment and training.
Establish and maintain in-line spinal.
If not breathing, begin positive pressure ventilations with pocket mask in the water if possible.
Float backboard under patient and move to shore if possible.
More thoroughly Evaluate responsive, airway, breathing, circulation once on land. IF HYPOTHERMIC A PULSE CHECK SHOULD LAST 30 TO 60 SECONDS BEFORE STARTING CPR.
- If pulseless and apneic go to Monitor/AED protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If hypothermic go to Hypothermia protocol.
- If head or spinal injury go to Spinal Injury/Head Injury protocols.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
Always transport submersion patients.
Pre-OB
Pre-Delivery Obstetric Emergency Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- IV
- Fetal Heart Rate
- Fundus measurement (can be palpated starting at 12 weeks just above pubic bone)
Evaluate responsive, airway, breathing, circulation
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
Patient positioning
- If conscious and alert place in POC. Possibly knees flexed if abdominal pain present.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place on left side.
- Most practical deliver position: Supine with knees drawn up to chest.
If patient is pregnant, check for crowning or abnormal presenting part
- If crowning go to Active Labor and Delivery protocol. If abnormal continue with this protocol.
If an abnormal presenting part is found, such as a prolapsed cord, hand, or foot, perform the following: Position patient in knee-chest position or elevate buttocks using pillows.Nuchal Cord If both feet or butt, prepare for deliver. Watch: Breech Delivery Video
- Head will be the main concern. Ensure the cord is not pinched off by the head. Place a gloved hand in the vagina and push the head away from the cord. This also allows for an air space for baby. If head does not deliver in 3 to 5 minutes transport and call medical control.
- “From the book” Transport immediately upon recognition of any complications of a breech delivery. Administer oxygen to the mother, and keep the mother in a supine head down position with her pelvis elevated so gravity will discourage the movement of the fetus into the vaginal. If delivery cannot be slowed contact medical control for assistance to deliver or continue to transport.
If umbilical cord is prolapsed
- Insert gloved hand into vagina and push presenting part of fetus away from cord. Cover presenting part with sterile mist dressing. Rapid transport patient and notify receiving facility of situation.Knee chest position
If vaginal bleeding is present (abortion less than 20 weeks),
- First or second trimester place a sanitary napkin over vaginal opening.
- Any female with abdominal pain especially in low quadrants must role out tubal pregnancy if occurring in first trimester.
- Do not insert anything into or pack the vagina. Save tissue, save underwear. Provide emotional support and transport.
Go to Active Labor and Delivery protocol, if birth is imminent. Once fetus is delivered go to Newborn Infant protocol Transport.
- If delivery is imminent pull over and deliver unless medical control advises otherwise.
Perform ongoing assessment every 5 if unstable and 15 if stable.
No need to ever in EMS do a pelvis internal exam on a female.
Active Labor and Delivery
Active Normal Labor and Delivery Drugs that might be useful:
- Terbutaline 0.25mg to delay contractions.
- Oxytocin 10 units IV to control post fetus/placenta delivery bleeding.
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- IV
- Fetal Heart Rate
- Fundus measurement (can be palpated starting at 12 weeks just above pubic bone)
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If abnormal fetus presentation go to Pre-Delivery OB protocol.
Patient positioning.
- If conscious and alert place in POC. Possibly knees flexed if abdominal pain present.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place on left side.
- Most practical deliver position: Supine with knees drawn up to chest.
Delivery imminent.
- Place patient supine with knees drawn up and check for crowning.
If crowning, contractions are 2 minutes apart, duration is 45 to 60 seconds long, urge to push, prepare for delivery Check for abnormal presenting part go to Pre-OB protocol. Prepare OB kit and create sterile field. If amniotic sac still intact, rupture and remove from fetus’ face. Head delivered look for cord. Slip over head and if not possible clamp in 2 places and cut.
- Watch: Nuchal Cord Video
Suction mouth then nose of infant Continue with delivery until expelled Keep infant level with mother Go to Newborn Infant protocol Clamp the cord in 2 places (6 inches from baby then 2 more) then cut cord) Deliver placenta. If greater than 10 minutes begin to transport.
- Watch: Placenta Delivery Video
Postpartum bleeding after delivery. Watch PPH Video
- Place a sanitary napkin over vagina after placenta is delivered.
- If still bleeding place baby on mothers breast and suckle.
- If still bleeding perform uterine messages on abdomen.
- Paramedic:
❖ 10 to 20 U of Oxytocin, IM or Piggyback.
❖ IV x2 for blood loss.
Ongoing assessment 5 unstable or 15 minutes if stable
Newborn Infant
Newborn Infant Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Apply SpO2
- Test glucose (heal stick)
- APGAR score
- Provide warmth
- If you suspect generalized cold emergency go to Hypothermia protocol.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
If meconium is present, aggressively suction airway until clear. Use suction machine if available not bulb syringe. Try to avoid over stimulation of baby to breathe until meconium removed.
Dry newborn with towels. Wrap newborn in warm towels or blanket. Be sure to cover head. Position newborn on back or lateral recumbent if large amount of secretions. Stimulate newborn by rubbing its back or flicking soles if breathing if activity is inadequate. Perform APGAR score at 1 and 5 minutes. If breathing is inadequate perform positive pressure ventilation with O2 for 30 to 60 seconds. Assess pulse.
- If heart rate is over 100 a minute assess color.
- If heart rate less than 100 but greater than 60 give 40 to 50 ventilations per minute for 30 to 60 seconds.
- If heart rate still less than 100 continue BVM until rate exceed 100 a minute.
- If heart rate is less than 60 begin CPR.
❖ Refer to CPR Chart Protocol.
Continue to reassess every 5 minutes even if stable. Support ABC, suction, dry, warm as needed. Newborns can deteriorate rapidly. Transport AHA PALS InvertedNote: Remember inverted pyramid:
- Warm dry suction, stimulate
- Basic oxygen delivery
- Aggressive oxygen delivery
- CPR
- Medications
Note: Ventilations and respirations of infant:
- Normal fluctuation is from 25 to 50 breaths per minute (can visit 60 a minute momentarily). If staying around 25 a minute stimulate. If they are staying at 60 or above provide override respiratory support and BVM to slow down rate to 40 to 50 breaths per minute.
- Grunting, see saw, or bobbing of head represents Respiratory failure. BVM them.
Note: Only use newborn equipment on newborns. Note: BVM should not have a working pop-off valve.
CPR Chart
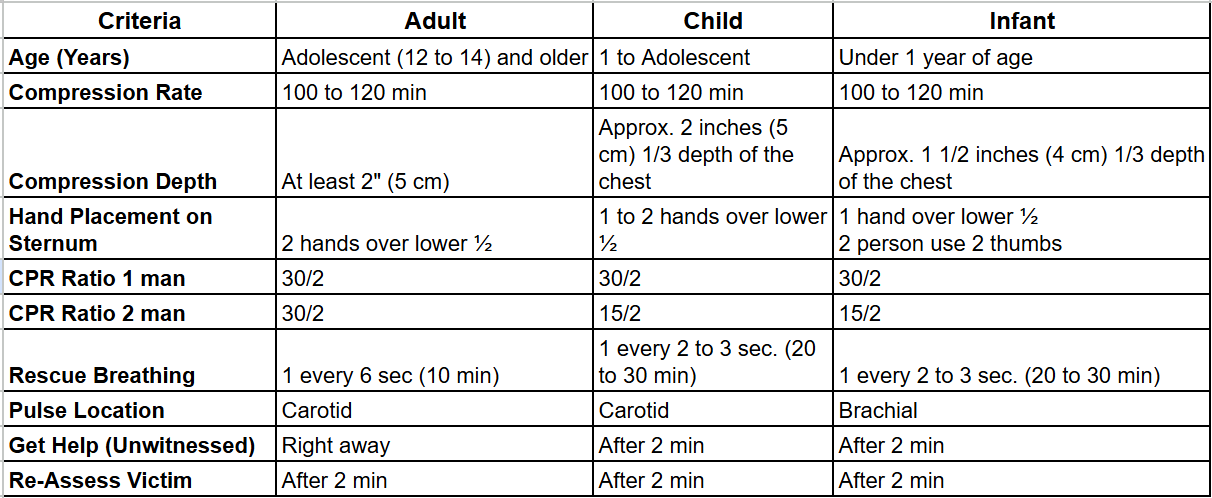
- If advanced airway (intubated, LMA, CombiTube) is placed do not have to synchronize compressions and ventilations.
- Conscious Chocking for over 1 year of age, do just like adult – 5 abdominal thrust in and up motion from behind and 5 back slaps/blows.
- Conscious Chocking less than 1 year of age – deliver 5 back blows (back slaps new term) and 5 chest thrust.
- Unconscious Choking over 1 year of age – treat like a cardiac arrest but just prior to ventilations look for obstruction.
- Unconscious Choking less than 1 year of age – treat like a cardiac arrest but just prior to ventilations look for obstruction.
- Never sweep an unconscious adult, child or infant for an object if you cannot see it.
- AHA Chain of Survival for adults – early help, early CPR, early defibrillation, early advanced care.
- AHA Chain of Survival for pediatrics – prevention, CPR, help, advanced care.
REVIEW THE CARDIAC MONITOR AND AED PROTOCOL.
Pediatric Respiratory Emergencies
Respiratory Emergency in the Infant or Child
Establish and maintain airway in sniffing position. If you find a child unresponsive just like an adult always open the airway with spinal precautions.
If complete foreign body airway obstruction suspected perform the following:
- Infant – head down, 5 back slaps then 5 chest thrust (or vise versa). Assess mouth finger sweep if object seen. Repeat if needed. After two sets transport and continue enroute.
- Child – Deliver 5 abdominal thrusts. Repeat twice if needed. After total of 10 abdominal thrust transport and continue enroute.
- Remember you get two sets then load and go and do more enroute.
If productive cough/cry partial obstruction place on oxygen and monitor for ineffective cough then do choking skills.
If respiratory failure, arrest, or inadequate breathing provide positive pressure ventilations at a minimum of 20 per minute if partial obstruction.
NO HUMAN (EVEN A NEWBORN) SHOULD BE BREATHING AT 60 A MINUTE OR MORE. OVERRIDE BVM AND SLOW DOWN. See General Difficulty Breathing protocol.
BLS should consider meeting up with ALS.
Expedite transport. Always try to keep the child and parent together in arms reach. Place parent on stretcher with child on lap, if possible, and safety belt both onto stretcher with own seatbelts.
If you suspect epiglottitis in a 3 year old to 7 year old do not try to visualize the oral cavity.
If you suspect croup in a 3 month to 3 year old you should hear stridor. High pitched sound heard in inhalation.
POC protect airway and humidify oxygen delivery.
Croup:
- Racemic Epinephrine 0.5mL of 2.25% nebulizer.
- 0.6mg/kg Dexamethasone IV up to 10mg in pedi patient.
Epiglottitis:
- Do not attempt intubation in field unless acute airway obstruction is present.
- If unable to intubate then cricothyroidotomy is next line of treatment.
Perform ongoing every 5 minutes stable or unstable in pediatrics
Soft Tissue Injuries
Soft Tissue Injury
Maintain manual c-spine support if head and neck injury suspected or unknown
Evaluate responsive, airway, breathing, circulation
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If bleeding or shock go to Bleeding and Shock protocol.
Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
Control any major life-threatening bleeding
- Non-Multisystem trauma:
❖ Direct pressure, elevate, pressure point (femoral or brachial only), tourniquet (last resort).
- Multisystem trauma:
❖ Direct pressure then move to tourniquet.
Maintain body temperature and keep patient calm
If open chest injury (sucking chest wound)
- Apply non-porous dressing. Secure on three sides and make a flutter dressing. Or secure of all four side. For testing purposes if you have to pick between taping 3 or 4 sides always pick 3 sides.
- Airway priority. Once securing the airway and ensure adequate ventilations, place a gloved hand over the chest wound until an occlusive dressing can be applied.
- If respirations deteriorate after placing occlusive dressing, unseal while patient exhales.
- Paramedic Care:
❖ Needle decompression
➤ 2 and 3 intercostal space midclavicular
➤ 5 and 6 intercostal space midaxillary
❖ If suspected hemo do not decompress. If hemo is tapped close needle.
If abdominal bleed with tenderness and/or pelvic pain
- Consider PASG. See Bleeding and Shock protocol for indications and contraindications.
➤ PASG can provide direct pressure.
If evisceration
- Apply moist sterile dressing and flex knees if possible.
- Do not contaminate.
- Do not replace organs.
If large neck laceration
- Control bleeding and apply a non-porous dressing.
- While securing airway place a gloved hand over the neck wound.
If impaled object
- Apply dressing to wound and then stabilize the impaled item in place.
- Remove only if impaled in cheek and obstructing airway. Removing object in same direction it entered. Reverse the path.
If avulsion
- Partial – Rinse wound to clean off debris if necessary.
- Partial – Apply dressing and bandage to keep avulsed tissue in place.
- Complete – treat as amputated part.
If amputation (partial)
- Realign extremity to as normal as possible.
If amputation (complete)
- Control bleeding and treat patient first.
- Wrap part in sterile dressing place in bag and place in cool place.
If bitten by vector borne (animal) or humans
- Should always be advised to seek medical attention.
- Perform emergency move if scene is not safe to EMS and patient.
- Wash the wound with soap and water.
- Dress with a dry dressing.
Transport. Golden hour 10 minute on scene time
Ongoing assessment 5 unstable or 15 stable
Pain management, as needed
- Morphine 2-4mg IV max 10mg.
- Fentanyl 50 – 200 mcg IV or IN.
Burn Injuries
Burn Emergency
Remove patient from burning source and stop burning if safe to do so.
- Stop/drop/roll, smother, water….
- Remember infection kills. EMS should wear entire PPE available.
Maintain manual c-spine support if head and neck injury suspected or unknown
Evaluate responsive, airway, breathing, circulation. ECG, IV’s, Blood Sugar
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General SOB protocol to maintain airway if needed then return to this protocol.
- Aggressive airway management of evidence of inhalation injury.
- If bleeding or shock go to Bleeding and Shock protocol.
Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
Estimate severity of burn
- Body surface area (BSA) using rules of 9.
- Estimate depth of burns.
- Priority burns: Less than 5 years of age and over 55 years of age. Burns to feet, hands, groin, chest, face. Inhalation burns, and circumferential burns.
Apply sterile dressing and bandage or burn sheet
- Keep loose because of swelling.
If BSA less than 10% dress wet.
- Dress all other burns dry. When in doubt keep dry.
Maintain body temperature
If IV emergency fluid resuscitation is needed to maintain perfusion.
- Parkland Burn Formula
- 4mL/kg of body weight times % BSA burned (2nd &3rd degree only) will be the fluid given during the first 24 hours. (formula is: 4X weight X Burned %).
- Give half of this amount during the first 8 hours from the time of injury.
- Lactated Ringers is the preferred fluid.
Pain Management
- Morphine 2-4mg IV max 10mg.
- Fentanyl 50 – 200mcg IV or IN.
Manage other associated injuries
Dry chemical burn
- Brush off and remove clothing and flush for 20 minutes.
Liquid chemical burn
- Remove clothing flush 20 minutes.
Chemical burn to eyes
- Flush 20 minutes
- Open eye lids unless fused closed and flush.
Thermal burns to eyes
- Do not open eyelids.
- Apply moist sterile dressing to both eyes.
Electrical burns
- If cardiac arrest suspect V-fib.
- Apply ECG monitor.
- Monitor pulse and respirations.
- Look for entrance and exit wounds.
- Look for pathway (entrance and exit wounds). Foot to foot, foot to arm, arm to arm most common.
Ongoing assessment 5 unstable and 15 stable
Musculoskeletal Injuries
Musculoskeletal Injury
Maintain manual c-spine support if head and neck injury suspected or unknown
- Evaluate responsive, airway, breathing, circulation
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If bleeding or shock go to Bleeding and Shock protocol.
Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
Dress/bandage all open wounds prior to splinting
If fracture is grossly deformed or no distal pulse
- Apply gentile traction and attempt to realign.
- If excruciating pain or resistance is met, stop and splint in the position found.
Splint suspected dislocations and knee
- Splint in position found unless no pulse present.
Hip dislocation or fracture
- Pad between both legs and bind together.
- Or apply long board splints and place on back board.
- Or pelvis apply PASG inflate all three sections to splinting pressure.
- Or pad between legs and bind legs together and place on back board.
Femur Fracture
- Must be isolated mid-shaft femur fracture for traction splint.
- If using PASG with traction splint, the PASG goes on first then traction over PASG.
- Apply traction splint and then back board to move.
Upper extremity injury
- Shoulder sling and swathe.
- Move arm to normal position if possible.
- Place hand in position of function if possible.
Always reassess PMS and document
Transport
Ongoing assessment 5 unstable and 15 stable
Pain management, as needed
- Morphine 2-4mg IV max 10mg.
- Fentanyl 50-200mcg IV or IN
Eye Injuries
Eye Injury
Maintain manual c-spine support if head and neck injury suspected or unknown
Evaluate responsive, airway, breathing, circulation
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If bleeding or shock go to Bleeding and Shock protocol.
Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
Foreign object in eye
- If possible transport patient for further evaluation and removal of the object by emergency department staff.
- Only attempt to remove non-embedded objects on the conjunctiva.
- Do not attempt remove of objects on or lodged in the cornea.
- No not administer anesthetic drops if outer layers have been ruptured.
- To remove a foreign object from the conjunctiva flush with water.
- If not successful and under the upper lid, draw upper lid down over lower lid.
- If object remains lift lid with cotton swab and remove with corner of sterile gauze or swab.
Orbital injury if eyeball not injured
- Place ice packs over injured eye.
- If eyeball injured do not use cold packs.
- Refer to Globe injury below.
Lid injury control bleeding
- With light pressure control bleeding.
- Do not use pressure if eyeball is injured also.
- Cover lid with sterile gauze in saline.
- No not administer anesthetic drops.
Preserve avulsed skin and transport with patient if needed
- No not administer anesthetic drops.
If eyeball injury is not suspected
- Cover lid with cold compress, patch both eyes.
- If irritation administer anesthetic Tetracaine 1-2 drops ever 15 minutes as needed.
❖ Due to preservatives in Tetracaine eye may burn for a few seconds prior to numbing effects.
Injury to the globe
- Apply patches to both eyes.
- Do not apply pressure.
- Apply a eye shield to injured eye.
- Keep patient supine.
- No not administer anesthetic drops.
Chemical burn to eye
- Irrigation with water for 20 minutes.
- Do not contaminate uninjured eye.
- Force lids open if needed to flush.
- If irritation (example mace) administer anesthetic Tetracaine 1-2 drops ever 15 minutes as needed.
Remove contact lenses
- If not going to aggravate the wound remove contacts.
Transport
Ongoing every 5 unstable and 15 stable
Head Injury
Head Injury
Signs/Symptoms: Hallmark sign is altered mental status.
- Maintain manual c-spine support if head and neck injury suspected or unknown.
- Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty protocol to maintain airway if needed then return to this protocol.
- If bleeding or shock go to Bleeding / Shock protocol.
Patient positioning.
- If trauma place on backboard.
- If low BP or unresponsive place supine and elevate legs.
- If BP normal/to high elevate head 15 degrees.
When controlling bleeding be careful not to apply excessive pressure to a open skull fracture.
Elevate head 8 to 10 inches if BP is acceptable.
Transport. Golden hour 10 minutes on scene.
Be prepared for Cushing’s: Slow pulse, high BP, erratic respirations, projectile vomiting, widening pulse pressure.
Be prepared for seizures. Go to Seizure protocol.
Ongoing every 5 unstable and 15 sable.
Avoid Nitro, Glucose.
Helmet removal:
- If good fit, no need to assess head, and can immobilize in a neutral position leave helmet on.
- If not good fit, you need to do airway skills, or cannot immobilize in a neutral position remove helmet.
Note: If patient meets the criteria to BVM in the General SOB protocol consider hyperventilating the head injured victim at about 24 breaths per minute (35 to 40 torr ETCO2) to blow off CO2. If posturing is present ventilate to 30 to 35 torr ETCO2.
Spine Injury
Spinal Injury
Signs/Symptoms: Best signs are paralyzed, numbness in extremities.
Maintain manual c-spine support if head and neck injury suspected or unknown.
Evaluate responsive, airway, breathing, circulation.
If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
If bleeding or shock go to Bleeding / Shock protocol.
Patient positioning.
- If trauma place on backboard.
- If low BP place supine.
Immobilization devise.
- Place on long board if unstable. Use a minimum of 3 straps. Secure torso then head.
- Place in short board (KED) if stable and found in seated position. Secure torso then head then place patient on long board for transport.
- If you find them walking at the scene stop movement immediately and long board in a standing position.
- Note: When placing a cervical collar evaluate the neck prior to covering. Advise conscious patient it is going to be unconfortable.
- Check PMS prior to placement and throughout transport for changes.
Shock.
- If BP and heart rate slow or regular, skin pale and cool, and clammy think neurogenic shock. Go to Bleeding / Shock protocol.
- If BP low and heart rate fast suspect hypovolemic shock. Go to Bleeding / Shock protocol.
- Transport. Golden hour 10 minutes on scene.
- Ongoing every 5 minutes if unstable and every 15 minutes if stable.
Note: Spinal immobilization is required for the following:
- Significant MOI who have an altered LOC, intoxicated, complain of head-neck-back pain.
- Significant trauma above the nipple line.
- Symptoms of neurological injuries.
- Tenderness to neck-spine with palpation.
- Penetrating injury: Strong suspicion of spinal injury based on location of injury.
Chest Injury
Chest Injury
Maintain manual c-spine support if head and neck injury suspected or unknown.
Evaluate responsive, airway, breathing, circulation.
If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
If bleeding or shock go to Bleeding / Shock protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
If obvious open chest wound.
- Place glove hand over wound until non-porous material dressing is used.
- If open chest wound is occluded with a dressing and patient suddenly begins to deteriorate, lift dressing off wound during exhalation to relieve trapped air then reapply dressing. Also see Soft issue Injury protocol.
Impaled object stabilize in place after controlling bleeding.
Flailed segments/ non-intact chest wall.
If inadequate breathing begin positive pressure ventilation. If available BVM may have limited use. If Positive Flow Ventilator (40+ LPM) is available use it.
Place glove hand over broken segment then stabilize with blanket, pillow, bulky dressing.
Do not use sand bags / IV bags to splint flailed segments.
Transport.
Ongoing every 5 minutes if unstable and every 15 minutes if stable.
Facial Injury
Facial Injury
Maintain manual c-spine support if head and neck injury suspected or unknown.
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If bleeding or shock go to Bleeding / Shock protocol
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
- Be careful not to apply excessive pressure to an open skull fracture.
- Apply a moist dressing to any exposed tendons, ligaments, or exposed bones.
- Avulsed tooth.
Place in cup of sterile water or wrap in gauze soaked in saline.
Control bleeding from tooth socket with gauze pad.
Make sure the gauze pad does not become a choking hazard.
Optional storage of tooth: treat just like an amputated part in a cool place.
- Foreign object in cheek that did not penetrate completely through the cheek use bulky dressing to stabilize.
- Foreign object penetrated through to other side.
Remove in same direction it entered if interfering with airway control. Reverse the path.
Pack dressing between gums and cheek to control bleeding.
Injury to nose (Epistaxis).
- Lean forward, pinch, ice and spit out blood.
- Check BP in elderly patient, might be high.
- If patient has clotting problems transport immediately.
Injury to ear.
- Save avulsed parts.
- Do not probe or pack the ear.
- Place loose dressing to absorbed blood and fluid.
- No pressure.
- Do not try to remove an object in the ear.
Bleeding from ear or nose with head injury.
- Do not pack.
- Place loose dressing to absorb blood.
- Perform target (halo) test. If positive go to Head Injury protocol.
Transport.
Ongoing every 5 minutes if unstable and every 15 minutes if stable.
Bleeding and Shock
Bleeding and Shock
Evaluate responsive, airway, breathing, circulation
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If impaled object go to Soft Tissue Protocol
- If evisceration go to Soft Tissue Protocol
- If avulsion go to Soft Tissue Protocol
- If amputation go to Soft Tissue Protocol
Standard Care/Monitoring:
- Administer oxygen high flow.
- ECG
- SpO2
- ETCO2
- Establish 2 IV’s
- Keep patient warm.
- Minimize patient exertion.
Maintain manual c-spine support if head and neck injury suspected or unknown Evaluate responsive, airway, breathing, circulation Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
Control any major life-threatening bleeding that is multitrauma or severe bleeding. If direct pressure cannot maintain control go straight to tourniquet Isolated mild/moderate bleeding without multisystem trauma: Direct pressure, elevate, pressure point (femoral or brachial only), tourniquet (last resort) Maintain body temperature and keep patient calm If abdominal tenderness and pelvic pain indicating internal bleeding or large soft tissue injuries of lower extremities consider PASG for direct pressure and splinting.
- PASG contraindicated entirely for CHF / Pulmonary Edema patient.
- SEPTIC is when correct to use legs but not abdomen section. Systolic over 100mmHg, Evisceration, Pregnant in 2/3 trimester, Thumper used for CPR, Impaled object, Chest trauma that needs free movement of diaphragm.
- Note: If used for shock pump to 90mmHg. If used to control bleeding inflate for direct pressure but so not to interfere with PMS.
- NOTE: For lower leg fractures and bleeding (tibia and fibula) use the PASG if available. It will provide direct pressure and stabilize the region. Do not worry about bone ends popping the PASG if used for lower leg bleeding.
- Note: Inflate or deflate PASG only with medical control permission.
If shock, keep patient calm, give oxygen, keep warm, and elevate the feet Fluid replacement
- Low-resistance shock (anaphylaxis, septic, neurogenic) infuse 250mL IV boluses as needed to a max of 1 liter.
- Uncontrolled bleeding with shock deliver enough fluid to maintain a radial pulse (80-90mmHg).
- Pediatric: 20mL/Kg IV fluid x 3.
- Adult: Consult medical control once 500mL IV boluses start to total 20mL/kg. At this point fluid may bee diluting blood too much.
Cardiogenic shock
- BP of 70 to 90mmHg Dopamine 2-20mcg/kg/min.
- BP less than 70mmHg Levophed drip at 0.5-12mcg/min.
Ongoing every 5 minutes Transport
- Golden hour 10 minute on scene time. LOAD AND GO!
Patient Refusal
Patient Refusal of Treatment or Transport click here to view “refusal form”.
- Once a duty to act is present the goal of EMS is to transport the patient to the hospital.
- If patient asks EMS for advise if transport is necessary the response is, “we are unable to determine the need at this time.”
- EMS will follow patients request for transport even if transport is unnecessary.
Refusal Requirements
- Patient must initiate the refusal.
- Age of 18 years old or older (May be less depending on medical director and state).
❖ Exception
➤ Emancipated Minor Exception
➤ Legally Married Exception
➤ Pregnant Exception
➤ Active Military Service
- Patient must be A&Ox4
- Patient judgment not influenced by alcohol or drugs (prescription or recreational) use.
- Patient must have control of basic body functions. (stance, balance)
- Patient has no imminent feelings, plan or means of suicide.
- Patient vital signs within normal limits.
- Patient has no evidence of life or limb threatening injury or illness.
Granting Refusal
- A minimum of two on scene EMS professionals must agree.
- If above criteria is clearly met a refusal may be granted.
- If above criteria is questionable contact medical control.
Documentation of Refusal
- Complete standard patient evaluation forms.
- Document A&Ox4.
- Document that transport was offered and refused.
- Document age of patient.
- Document that a witness observed the situation. Obtain signature of witness. (Bystander, Family Member)
- Document that above criteria was met in full.
- Document signature of at least two on scene EMS professionals.
- Document that the statement was made that by EMS granting this refusal doe not suggest that there is no need to be seen by a doctor.
- Document the signature of patient. (A minor may not sign only the agent – parent, adopted parent, legal guardian, law enforcement).
Care Options
- Patient may consent to treatment but not transport.
- Patient may consent to transport but not treatment.
- At any time the patient may terminate consent if above criteria is met for granting refusal.
Family Violence
Family Violence
- Treat injuries and illness as necessary.
- Document observations and care provided.
- Must give the patient/victim referral information for family notice.
❖ Local police number
❖ Local shelters or social organizations and phone numbers.
❖ Advice the victim to seek legal aid.
❖ Provide notice in commonly used language of victim.
Info to be given to patient: Click here for: “Family Violence Form – English“. Also comes in Spanish.
Child Abuse and Elderly Abuse
Child and Elderly Abuse
Consider law enforcement to gain entry if scene becomes physically unstable or dangerous to abused patient or EMS.
If family members are allowing EMS to treat abuse patient and you suspect abuse advise receiving facility of your suspicions because a doctor is specifically trained to identify abuse.
Do not ask to recreate the situation or answer questions while still in the abusive environment.
Have a trained profession in abuse interview the patient. Not EMS.
Your main goal is assessment and treatment.
Do not questions the care givers about the abuse.
Do not let the abused patient be left alone with the abuser.
Provide accurate and objective documentation.
Do not allow abuser(s) to know EMS suspects abuse. Keep mouth shut. Do not show your cards to abuser!
Dead Upon Arrival and DNR
Dead upon Arrival
- Obvious expiration; rigor mortis, livor mortis (lividity), decapitation, visible brain matter, decomposition.
- Note: Warmth is not a determining factor.
- Multiple Casualty Incident – If pulseless at time of assessment – receive a black tag. If arrest after assessment receive a red tag.
- Preserve chain of evidence. Do not disturb the scene. Document anything your touch and move.
Do Not Resuscitate
- The form can be an original or exact copy.
- Must be the Texas-Out-of-Hospital DNR Form
❖ Click here for: Tx DNR Form
- Upon determining a valid DNR order the following are withheld or withdrawn;
❖ CPR
❖ Artificial Ventilation
❖ AED
- A “qualifying person” may override the DNR. (listed on back of DNR)
- If cardiac arrest is result of a crime or if pregnant the DNR does not apply.
- Contact medical control for assistance.
DO NOT DELAY CARE TO VALIDATE THE DNR. AS RESPONDERS ARRIVE AND RESOURCES PERMIT THEN VALIDATE THE DNR.
Pending Protocols
Collapse content goes here….
Airway Management and General Difficulty Breathing
Airway Management and General Breathing Difficulty
Establish and maintain open airway. No matter what the condition, the airway must remain patent at all times.
Head Tilt-Chin-Lift or Jaw Thrust Head Tilt Maneuver: No neck injury suspected. Head Tilt-Chin-Lift is temporary and must be replaced with an upper airway adjunct unless the patient begins adequate spontaneous ventilations. Indications: Any unresponsive patient without history of MOI. Cardiac arrest without MOI. Apneic patients without MOI.
Jaw Thrust In-line Maneuver: Used with suspicion of spinal injury. Use of a Jaw Thrust is temporary and must be replaced with an upper airway adjunct unless the patient begins adequate spontaneous ventilations. Indications: Unresponsive trauma patient. Unresponsive patient with an undetermined MOI.
Note: If difficult to ventilate or air will not enter always reposition the head and attempt ventilation again.
Suction secretions as needed.
Patient needs suctioned immediately when gurgling sound is heard with artificial ventilations. Suction devices may not be able to remove large obstructing particles in the airway. Roll patient to the side and remove manually large obstructions then follow with mechanical suctioning if needed.
If patient produces frothy secretions as rapidly as suctioning can remove, suction for 15 seconds, artificially ventilate for 2 minutes, and continue in that manner. Consult medical direction for this situation.
Assess quality, rhythm and rate of ventilations. Note: Mental status and/or cyanosis is not always a main determining factor to indicate need for oxygen. Look at rate, rhythm and quality to decide on the best oxygen device.
Signs of inadequate ventilator status (if patient is breathing). Adult: Rate less than 12 or greater than 20/minute. Rhythm irregular, such as taking a series of deep breaths followed by periods of apnea. Quality of auscultated breath sounds diminished, noisy or absent. Reduced flow of expired air out the nose and mouth. Chest expansion unequal or inadequate results in reduced tidal volume and minute volume. Increase effort to breathing using accessory muscles. Skin may become pale or cyanotic and cool and clammy with or without agonal respirations.
Techniques of artificial ventilation if needed.
The following patients need artificial ventilations: Any patient with reduces minute volume (breathing rate and depth). Respiratory arrest will require approximately 12 ventilations per minute. Reduces tidal volume and a rapid rate (hyperventilation) will need rate control. Reduced minute volume (hypoventilation) require rate and volume assistance.
- Hyperventilating not associated to hyperventilation syndrome (panic attack) patient: Explain procedure to responsive patient. Place mask over nose and mouth. Initially assist ventilate at the rate at which patient has been breathing. Over the next 5-10 breaths, slowly adjust the rate and deliver tidal volume until adequate minute volume.
- Hypoventilating patient: Place mask over nose and mouth. Initially assist ventilate at the rate at which patient has been breathing. Over the next 5-10 breaths, slowly adjust the rate and deliver tidal volume until adequate minute volume.
Special situations:
- Laryngectomies (stomas): Check for obstructions and suction. Upon artificial ventilations air escapes from mouth and nose, close the mouth and nostrils.
- Infants and children: Do not hyperextend the head. Do not use pop-off valve on BVM for infants/children.
- Dental appliances: Dentures should be left in place. Partial dentures may become dislodged. Leave in place, but be prepared to remove dentures if they become dislodged.
Equipment for artificial ventilations.
2 person BVM. Advantages good seal and two hands squeezing the bag. Disadvantage requires two rescuers.
1 person BVM. Advantage only one rescuer needed. Disadvantage requires a skilled rescuer. Only the highly skilled and frequent users are able to obtain and maintain an adequate mask to face seal.Flow Restrictive Ventilator
Flow restrictive, oxygen-powered ventilation device. Major advantages provides high concentration of O2 while allowing EMT to use 2 hands to maintain seal. Major disadvantage may not be used with all types of patients for example lung disease and children.
Mouth to mask with one way valve. Advantages one rescuer device.
Equipment for supplemental oxygen delivery.
Non-rebreather mask: Oxygen rate 10 to 15 liters. Do not go under 10 LPM with a non-rebreather mask.
Nasal cannula: Rarely the best method of delivering adequate oxygen to the hypoxic patient. Should only be used when patient will not tolerate a non-rebreather mask, despite coaching from healthcare professional.
Artificially ventilate versus Supplemental Non-Rebreather mask.
If initial assessment reveals respiratory distress as listed under number 3 then proceed to the following:
- PulseOx low
- ETCO2 high
- Tidal volume low
- Rate too low or high
If patient is responsive and the breathing is adequate (good rate, quality and volume) oxygen still may be indicated.
- PulseOx 94 to 100 = Room Air
- PulseOx 90 to 94 = NC 1-4 LPM
- PulseOx less than 90
❖ Good Tidal Volume NR 10-12 LPM
❖ Poor Tidal Volume BVM 15 LPM
If patient is responsive and the breathing is inadequate (poor rate, quality or volume) and assist the patient’s ventilation using methods listed in number 4.
If the patient is unresponsive and the breathing is adequate (good rate, quality and volume), provide high concentration oxygen non-rebreather.
If the patient is unresponsive and the breathing is inadequate (poor rate, quality or volume) use methods listed in number 4.
Defining mild, moderate and severe breathing difficulty.
- Mild (dyspnea): May be hypoxic but can move an adequate tidal volume. Can answer questions in sentences and alert. Administer non-rebreather. Start to treat underlying causes.
- Moderate (Mild Failure): May be hypoxic but can move an adequate tidal volume. Having difficulty answering questions. Wheezing can be a upper and lower whistling sound. Still awake but may be restless/irritable. May not let you assist breathing with BVM at this time. Administer non-rebreather mask. Get ready with BVM if needed. Start to treat underlying causes.
- Severe (Moderate/Severe Failure): Respiratory Failure is clearly present. Getting sleepy. Not speaking or speaking very few words. Patient usually sitting upright (tripod). BVM and timed with inhalation.
IF PATIENT BENEFIT FROM BRONCHODILATOR AND THE CLINICAL SIGNS INDICATE POSSIBLE BENEFIT FROM ITS USE:
CONSULT MEDICAL CONTROL ALWAYS FIRST.
- EMT – If patient has prescribed bronchodilator may be indicated to assist patient in delivery.
❖ Contraindications: Inability of patient to use device. Inhaler not prescribed for the patient. No permission from medical direction. Patient already met maximum dose.
- Paramedic
❖ albuterol 2.5mg/3mL Neb repeat once in 10 min or 90mcg x 2 MDI
❖ Atrovent 0.5mg/2.5mL Neb (Good for questionable heart condition)
❖ Xopenex 1.25mg/2.5mL Neb
❖ terbutaline 0.25mg SubQ
❖ Severe cases: May mix albuterol with Atrovent.
Insert airway Adjuncts if needed.
Nasopharyngeal airway: Less likely to stimulate vomiting. Measure nose to ear, lubricate with water-base, bevel to the septum. Examples of patient needing nasal airway: Unresponsive and snoring or unresponsive with gag reflex.
Oropharyngeal airway: Unresponsive patient without gag reflex. Measure from corner of mouth to ear or angle of the jaw. Adult rotate 90 to 180 degrees, pediatric depress tongue and place or rotate up to 90 degrees. Examples of patient needing oral airway: Unresponsive, apneic patients. Any apneic patient being ventilated with a BVM.
Benefit of OPA:
- Evaluate gag to assess if airway is protected.
- Keeps teeth apart for BVM
- Allows assessment for how wide mouth can be opened for intubation.
- Aids in suction of lower airway.
Transport in POC.
Perform ongoing assessment every 5 minutes
If patients ventilatory drive is failing, prolonged BVM or patient cannot protect airway consider advanced airway.
LMA – EMT & Medic skill
King Tube – EMT & Medic skill
CombiTube – EMT & Medic skill
- Contraindicated with esophageal varices
ETT Intubation – Medic Skill
If spontaneously breathing consider
- Nasal intubation with whistle tip to bypass gag.
- Conscious sedation intubation
❖ Ketamine 1-2mg/kg
❖ Propofol 2mg/kg
❖ Etomidate 0.3mg/kg
❖ Midazolam 1mg SIVP
❖ Then give a little narcotic – Fentanyl or Morphine
❖ Most common is Versed and Fentanyl
- Rapid sequence intubation (RSI) Watch Video: RSI
❖ Sedative
➤ Ketamine 1-2mg/kg
➤ Propofol 2mg/kg
➤ Etomidate 0.3mg/kg
➤ Midazolam 1mg SIVP
❖ Neuromuscular Blocker
➤ Vocuronium (ROC) 1mg/kg Adult – 100mg (Give before sedative)
➤ Succinylcholine 1mg/kg Adult 100mg (Give after sedative)
If positive pressure is needed in the lungs consider ETT (PEEP)
Cardiac Monitor and AED
Cardiac Monitor and AED Manual Cardiac Monitor:
- Defibrillation: Watch Defib Video
- Unconscious patient: Perform quick look to identify if V-Fib or V-Tach pulseless is present.
- Deliver 360J or biphasic energy range.
- Perform 2 minutes of immediate CPR.
- If patient is down for more than 4 to 5 minutes perform 2 minutes of CPR prior to defibrillation.
- Paddle / Hands Free Pads
AED Machine:
- AED PADS size: 0 to 8 years old use pedi pads provided with AED.
- If no pedi pads are available may use adult pads.
- Adults AED pads are for age 8 and above.
Manual Cardiac Monitor:
- Pedi paddle/pads are used on 10 kg (1 year old) and less.
- Studies show that hands-free provides quicker time to shock that paddles.
Note:
- If AED is analyzing let it perform as needed. Let AED deliver the first shock if needed. Then remove AED and place patient on manual cardiac monitor.
- Semi automated defibrillator is the same as an AED learned in EMS school. Semi just means the EMT has to at lease press one button.
- Primary shockable rhythms are Ventricular Fibrillation and Pulseless Ventricular Tachycardia.
- Prepare the patient for transport after no shock advised, or after patient regains pulse.
- If pulse is present then check breathing. If breathing or not refer to General Breathing Difficulty Protocol
- If AED is used keep it attached until ALS arrives then use manual cardiac monitor.
Pad/Paddle placement
- Place pads 1 to 2 inches away from implanted devices.
- Shave if needed.
- Remove medication patches.
- Chest must be dry.
- Avoid direct contact with metal.
Place pads/electrodes as advised.
- Most common placement: Pad 1 right of sternum below clavicle or breast. Pad 2 place 2 inches below left armpit.
- Anterior Posterior position: Left infrascapular under scapula other Left infraclavicular.
- Left and Right infrascapular
- Anterior Apex Left intrascapular
Synchronized Cardioversion: Watch Synch Video
- Patient is extremely rapid heart rate and cardiac in origin.
❖ Synch avoids R on T. Delivers electricity on QRS not the T wave.
❖ Use paddles/pads as stated above.
❖ 100J, 200J, 300J, 360J monophasic or equivalent biphasic energy.
➤ Check for pulse between each shock.
➤ In emergency titrate sedative for pain. Do not pre-load.
Transcutanious Pacing: Watch Pacing Video
- Used on bradycardic unstable patients.
❖ Pad selection as stated above.
❖ Unstable patient set rate to 80 beats per minute – set milliamps (mA) to 80. If no capture increase mA.
If capture present at 80 reduce and titrate.
❖ In emergency titrate sedative for pain. Do not pre-load.
Allergic Reaction
Allergic Reaction Signs and symptoms:
- Mild reaction normal vitals with urticaria (hives), itching.Urticaria
- Moderate reaction is mild reaction plus respiratory compromise.
- Severe reaction (anaphylaxis) has mild and moderate and now circulatory collapse.
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
❖ Never underestimate the severity of an allergic reaction. If breathing is adequate but likely to deteriorate rapidly, place patient on a non-rebreather at minimum care. Even if patient is only showing signs of a mild reaction. Due to potential of rapid deterioration be proactive, place on oxygen.
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Establish IV Large Bore
- Ensure scene is safe from bees, wasps, etc… Move patient to safety.
- Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor Protocol and/or CPR Chart Protocol.
- If breathing difficulty is present go to General Difficulty Breathing Protocol to maintain airway if needed then return to this protocol.
Care:
- If Mild (Localized Reaction) only:
❖ Benadryl 25mg-50mg IM or IV.
❖ Pedi: Benadryl 1mg/kg IV or IM.
- If Moderate Dyspnea, but SBP > 90mmHg without Shock, Hypoperfusion, or Critical Airway:
❖ Bronchdilate
➤ albuterol 2.5mg/3mL Neb repeat once in 10 min or 90mcg x 2 MDI.
➤ Atrovent 0.5mg/2.5mL Neb (Good for questionable heart condition).
➤ Xopenex 1.25mg/2.5mL Neb
➤ terbutaline 0.25mg SubQ
➤ Severe cases: May mix albuterol with Atrovent.
➤ Epi 1:1,000
✔ EMT: EPI-PEN 0.15mg (pedi) or 0.3mg (adult) IM
✔ Paramedic: 0.3-0.5mg SubQ
❖ Antihistamine
➤ Benadryl as listed in mild reaction.
❖ Steroids
➤ Dexamethasone 4-24 mg IV
➤ Solu-Medrol 60-250 mg IV.
✔ Pedi dose: Solu-Medrol 1-2mg/kg IV, Dexamethasone 0.25mg/kg IV.
- If Severe (Shock), Severe Hypoperfusion, Critical Airway or SBP < 90mmHg:
Supine position with legs elevated or trendelenburg position, if tolerated.
EPI
- EMT: EPI_PEN as described in moderate reaction.
- Paramedic Epi 1:10,000 0.3mg-0.5mg IV or 0.5mg 1:1000 sublingual injection: administer as soon as possible. Do not delay epinephrine sublingual injection administration while attempting IV access. Pedi dose: 0.01 to 0.1mg/kg IV 1:10,000.
Benadryl as stated in mild reaction.
250-1,000 ml fluid boluses and frequent reevaluation (may require 2 Liters)*. Pedi bolus: 20mL/kg x 3.
Steroids as described in moderate reaction.
Expedite transport
Perform an ongoing assessment every 5 minute
Paramedic: Prepare for need of intubation or surgical airway.
Seizure
Seizures
- If patient is actively seizing protect from the environment. Avoid physical restraint if possible.
- Only treatment possible while seizing is try treating the cause of the seizure:
examples:
❖ If diabetic seizing treat diabetes.
❖ If hyperthermia treat temperature.
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- Establish IV
Actively Seizing:
- 2 to 5mg valium IV slow or IM until seizure stops or max dose 10mg. Double dose if rectal.
❖ Pedi 0.1-0.5mg/kg
- 1 to 5mg Versed IV slow or IM.
❖ Pedi 0.1mg/kg
- 4mg Ativan IV slow. Not recommended for IM.
- Narcan 2-4mg IV or IM if seizure is of narcotic causes (rare).
❖ Pedi 0.1mg/kg
Hypoglycemic Seizures: (adult <60mg/dL – pedi <40mg/dl):
- D50 25-50g IV
❖ Pedi 1g/kg D25% or D10%
- If no IV Glucose Gel 25-50g Oral Mucus or Rectal
- If no IV Glucagon 1mg IM
- Note: If seizure actively stops after Glucose/Glucagon for diabetic seizures do not give Valium.
Once muscle convulsions have stopped:
- Evaluate responsive, airway, breathing, circulation.
❖ If pulseless and apneic go toAED/Cardiac Monitor protocol and/or CPR Chart Protocol.
❖ If breathing difficulty if present go to General SOB protocol to maintain airway if needed then return to this protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma suspected protect head and spine.
- If low BP place supine.
If febrile seizure
- Cool with tepid water.
- Pedi: Consider 15mg/kg rectal liquid Tylenol.
Note: Most common adult seizure reason is not taking anti-seizure medication. Transport
- If first time seizure
- Other underlining medical problem present
- If history of past seizures and not responding as expected like previous seizures transport.
Perform ongoing assessment every 5 minutes
Altered Medical Status - Diabetes
Altered Mental Status – Diabetic Emergency Signs and symptoms:
- Rapid onset of confusion. Unusual exercise. Staggered gate. Hunger. Seizure activity. Anxiousness, combative, or restlessness. Tachycardia. History of diabetes. Blood glucose of < 60 mg/dl (Pedi: <40mg/dl).
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- Establish IV
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If convulsions are present refer to Seizure protocol.
- If trauma suspected immobilize the patient and refer to Trauma protocols.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
Hypoglycemic: Glucose <60mg/dL (Pedi <40mg/dl)
- Sugar foods and drinks
❖ If conscious and alert, not nauseated or vomiting and can follow directions may give; water with sugar, fruit juices, soft candy (simple sugars).
- Glucose
❖ D50% 25-50g IV. (Pedi: 1g/kg D25% or D10%)
❖ Oral Glucose Gel 25-50g Oral mucus or rectal (Pedi 1g/kg)
- Narcan 2mg-4mg IV if no improvement with D50% (Pedi: 0.1mg/kg)
- Glucagon 1mg IM if no IV and unresponsive.
Non-Hypoglycemic: Glucose >80mg/dL
- Narcan 2-4mg IV, IM.
Note:
- Recent head injury contact medical control to see if relative contraindication at this time.
- If BS low and Glucose or Glucagon administration works do not give Narcan.
- If Glucose, Glucagon and Narcan do not work consider other causes of AMS
Transport Ongoing assessment every 5 minutes
Myocardial Infarction
Cardiac Compromise and Acute Coronary Syndromes Signs and Symptoms:
Chest pain/discomfort. Radiating pain to arms, neck, back. Sudden onset of sweating. Difficulty breathing. Cool, pale skin. Light headed, Anxiety or irritability. Feeling of doom. Abnormal or irregular pulse rate. Abnormal blood pressure. Nausea and/or vomiting.
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- Establish IV
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
- If pulmonary edema is present or possible use caution when lowering the head and evaluate breath sounds often.
Adult Care:
- Aspirin 160-325mg PO (chew and swallow).
❖ EMT may concider ASA with medical control permission.
- Obtain 12 lead ECG within 5 minutes of arrival.
❖ If Inferior Infarction (Leads II, III, aVF).
➤ Perform right sided 12 lead or 15 lead to role out inferioposterior MI.
✔ 15 lead (r/o posterior involvement)
▪️ Lead V4R: 5th IC space midclavicular on right side
▪️ V8: 5th IC space midscapular line
▪️ V9 goes between V8 and the spine
▪️ Place Lead V5 wire on V8 and V6 wire on V9. Attach V4 wire to the V4R position
✔ Confirm RV Failure is not present before Nitro/Morphine.
- If BP <90mmHg
❖ give 250mL fluid bolus IV if no pulmonary edema is present, titrate BP to >90mmHg.
- If BP >90mmHg
❖ Nitroglycerin SL 0.4mg up to 3 doses every 5 minutes.
➤ EMT: If patient has prescription contact medical control prior to assisting.
❖ If pain continues after nitro give:
➤ Morphine 2-4 mg increments to max 10mg IV-Slow. (Best drug)
➤ Fentanyl 50mcg IV Slow (Does not lower BP like Morphine)
➤ Nitrous Oxide self administered. (Good for pain with low BP)
➤ If N/V develops
✔ Phenergan 6 to 12mg IV Slow push
✔ Zofran 2-4 mg IV
- If BP extremely low consider vasopressors Dopamine or Levophed for cardiogenic shock.
Note:
- Contraindications Nitro and Morphine: Absolute contraindication if BP less than 90mmHg.
- Recently taken Viagra, Silderafil, Cialis, Tadalafil, Levitra, or Vardenafil within 24 hours do not administer Nitroglycerin unless advised by contact medical control.
- Nitroglycerine may take up to 2-3 minutes for full action. This is why you wait 2-3 minutes then take BP before you decide on another dose.
Record time and vitals
- 2-3 minutes after each drug given.
Do not unnecessarily delay transport.
- Keep patient calm.
Clot buster medication goal time is within 1 hour of onset of symptoms Ongoing assessment every 5 minutes
Stoke
Altered Speech, sensory, motor function – STROKE Emergency Signs and symptoms:
Cincinnati Stroke Scale: Arm drift, speech, facial droop. Confusion, poor balance, intoxicated appearance.
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Take BP in both Arms.
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- Establish IV
- 12 Lead
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
Patient positioning.
- If conscious and alert place in POC. Preferably semi-fowlers position.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
Speak to the patient and explain all procedures.
- Many times they may appear unresponsive but can hear your words.
Contact receiving hospital early to meet 3 hour window for clot busters. Avoid unnecessary oral glucose and nitro if a stroke is suspected.
- If hypoglycemic go to Diabetic protocol.
Perform ongoing assessment every 5 minutes. Blood Pressure
- Do not treat BP unless over 220/110.
❖ Labetalol 10mg IV
Note: If low BP present consider another cause for AMS.
Behavioral Emergency
Behavioral Emergency Ensure your safety and prepare for possible violence.
- Always have a partner.
- Do not rush the call.
- Keep your back to the exit.
- Call for law enforcement if needed for safety.
- Look at surroundings when you enter.
- Look at patient body language.
- It is not abandonment to leave an unsafe scene if patient contact has already been established.
Role Out Other Causes for AMS Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing protocol
- Test glucose
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If blood sugar low go to Diabetes protocol.
- If poison or drug overdose go to Poison protocol or Drug/ETOH protocol and then return to this protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
- Avoid letting the patient walk to ambulance. Elopement risk.
Assess patient for possible self inflicted injury. Patients are good at hiding injuries. Establish and maintain in-line spinal if suspected injury from hanging or trauma If patient is responding keep them calm.
- Do not rush.
- Do not give into their hallucinations.
- Get their psychiatrist staff or family member on the phone or to the scene.
If patient become violent and threatens physical harm to self or others restrain.
- May not restrain verbal abuse only physical.
Ongoing assessment every 5 unstable every 15 stable Do not leave patient alone Suicide risk.
- Any person can commit suicide.
- Look for the person with the means and the plan.
- Do they have a gun, or drugs to overdose on, or a plan.
May restrain if physical danger to self or others
- Use soft restraints 4 point
- Tie to bed not handrail
- Monitor ECG
- Pulse-Ox
- Document airway and PMS in restrained extremities every 5 minutes.
If needed Haldol may be given to calm patients
- Contact medical control for dosing.
Transport
- Do not allow them to walk to ambulance. Insist they are placed on the stretcher with all safety straps secure.
- Allow them to bring any personal item if they feel more comfortable.
- Listen to them. This is mental not physical. If they are not talking you cannot figure out how to help them.
Refusal:
- May not refuse even if A&Ox4 if you think they will carry out a plan of suicide.
- With medical control permission you may leave them with a family member. But only with medical control permission.
Recognize signs of stress for EMS workers
- Lack of sleep, drinking alcohol, lack of sex, depression, guilt, drugs.
- If an EMS worker shows signs they should be directed to a stress management course. Look out for each other.
Heat Emergencies
Heat Emergencies Remove from hot environment and/or humidity. Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- IV x 2 Large Bore
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If seizure go to Seizure protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
Turn up air conditioner to maximum. Remove excessive clothing. Heat Exhaustion or Heat Cramps: If skin is cool, moist, and pale (heat exhaustions) cool patient with wet compresses, fan, place supine raise feet. If not N/V give water by mouth 1-2 glass every 15 minutes. Monitor ECG, D-stick, IV fluid 500mL over 15 minutes. Heat Stroke: If skin is hot and dry (above 104 degrees) or even moist (heat stroke) pour water over patient, place cold packs in armpit, groin, fan patient. Tap a fire hydrant and soak patient. Just get the temperature out of the danger zone by any means possible. Key for heat stroke vs heat exhaustion is low BP.
- When pt starts to shiver slow the cooling process. IV fluid 500mL bolus x 3 does not acutely overload hydrate.
- Prepare for possible seizure activity. Go to Seizure protocol.
Transport Perform assessment every 5 minutes.
Hypothermia - Generalized
Generalized Cold Emergency – Hypothermia
Note: Never give up until they are warm, and dry. Only then are they dead.
Remove from cold environment. Prevent further heat loss.
Evaluate responsive, airway, breathing, circulation.
Standard Care/Monitoring:
- Pulse check should last a minimum of 30 seconds to 60 seconds before starting CPR.
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- IV
Protocols
- If you suspect localized cold emergency (frost nip/bite) with no general hypothermia go to Cold Injury protocol.
- If pulseless and apneic go to AED/Cardiac Monitor protocol
❖ If severely hypothermic deliver only one shock for V-Fib and perform CPR.
❖ Contact medical control for further orders.
- If severely hypothermic contact medical control prior to administering any drugs.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
❖ Warm and humidify the oxygen being delivered.
❖ Warm/hot packs not on body but within the blankets.
❖ Warm IV bags to 96-104 degrees.
Patient positioning.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
- Avoid rough handling and do not allow to walk around.
- Keep them flat. Tilting patient may lead to cardiac arrest V-Fib.
Remove all wet clothing, jewelry, etc…
If patient is alert and not confused begin to actively rewarm. Examples: Drink warm liquid not caffeine or alcohol.
Do not allow to eat or drink stimulants. Caffeine and alcohol are most common not to allow.
Do not rub.
Have AED/Cardiac monitor ready for V-Fib.
- If severely hypothermic only provide one 360J shock in V-fib until body temperate rises.
- Also withhold drug therapy until body temperature rises. Check with medical control prior to additional electric therapy and drug therapy.
Transport horizontal position. Backboard may be needed.
Perform ongoing assessment every 5 minutes.
Localized Cold Injury
Local Cold Injuries – Frost Nip and Frost Bite
Remove patient from the cold environment. Frost bite toe 2Frostbite toe
Standard Care/Monitoring:
- Pulse check should last a minimum of 30 seconds to 60 seconds before starting CPR.
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- IV
- If you suspect generalized cold emergency go to Hypothermia protocol.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
- Note: Avoid rough handling and do not allow to walk around.
Remove all wet clothing, jewelry, etc…
Cover affected frost nip/bite skin with dry sterile dressings.
If early; Frost Nip:
- Immobilize affected extremity, do not rub, do not re-expose to cold.
If late; Frost Bite:
- Do not rub, do not break blisters.
- Do not apply heat to rewarm.
- Do not allow them to walk on extremities.
- Try to separate fingers and toes unless already frozen together.
If required / instructed by medical control to rewarm:
- Immerse tissue in 104 degree water.
- Keep water at constant temperature.
- Keep immersed until color and feeling return to normal.
- Dress wound and protect from refreezing.
- Pain management
❖ Morphine 2-10 mg IV
❖ Fentanyl 50 to 200 mcg IV, IN
Transport
- Advise receiving facility to allow for equipment set up in ED.
Poisoning
Poisoning Emergencies
Protect yourself.
Evaluate responsive, airway, breathing, circulation.
If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
If allergic reaction go to Allergic Reaction protocol.
If seizure go to Seizure protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma protect head and spine.
- If low BP place supine.
Contact medical control and/or poison center for directions with treatment.
Ingested: IF PATIENT NEEDS ACTIVATED CHARCOAL AND THE CLINICAL SIGNS INDICATE POSSIBLE BENEFIT FROM ITS USE:
ALWAYS CONSULT MEDICAL CONTROL FIRST.
Facilitate administration of activated charcoal.
Indications (meets all of the following): Exhibits signs and symptoms of ingestion overdose/poisoning emergency. Specific authority by medical direction.
Dose: Activated charcoal 1g/kg or about 30-100g for adults and 12.5 to 25g for children.
Contraindications:
- Nauseated prior to administration.
- Ingestion consumed over 1 hour ago.
- Cannot swallow or follow instructions.
- Do not administer in acid or alkali poisoning.
- Avoid alcohol, kerosene, gasoline, metal poisoning because charcoal will not bind.
- No permission from medical direction.
- Patient already met maximum dose.
Side effects: Black stool, nausea /vomiting.
Note: Syrup of Ipecac is usually not given to ingestion overdoses/poisonings in EMS. Must be given within 20 to 30 minutes of ingestion. If patient becomes unresponsive will still vomit leading to an airway concern. Dose: 30mL in 8 oz glass of water.
Inhales:Remove from environment. High concentration of oxygen. Go to General Difficult Breathing protocol.
Injected: Scrape stinger from site. Wash injection site with soap and water. Watch for allergic reaction. Go to Allergic Reaction protocol.
Absorbed: Brush off dry chemicals, remove clothing and flush for at least 20 minutes.
If organophosphate poisoning.
Signs and symptoms of SLUDGE – Salivation, Lacrimation, Urination, Defecation, GI irritability, Eyes constrict.
Poisoning will stimulate parasympathetic stimuli.
Pesticides, fertilizers cause organophosphate poisonings. Think Nerve Gas.
Most commonly absorbed through skin. Irrigate skin.
Atropine is drug of choice – 2 to 5 mg loading dose may repeat.
EMT should consider ALS back-up on all overdoses/poisoning if unstable.
Potential for seizures. Go to Seizure protocol.
Transport.
Perform ongoing assessment every 5 minutes.
Drug or Alcohol Emergency
Drug or Alcohol Emergency
- Protect yourself from violent patients. Keep your back to the exit. Never be alone.
- Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine and elevate legs.
Contact medical control and/or poison center for directions with treatment.
Ingested pills/solids: IF PATIENT NEEDS ACTIVATED CHARCOAL AND THE CLINICAL SIGNS INDICATE POSSIBLEBENEFIT FROM ITS USE:
ALWAYS CONSULT MEDICAL CONTROL FIRST.
Facilitate administration of activated charcoal.
Indications (meets all of the following): Exhibits signs and symptoms of ingestion overdose/poisoning emergency. Specific authority by medical direction.
Dose: Activated charcoal 1g/kg or about 30-100g for adults and 12.5 to 25g for children.
Contraindications: Nauseated prior to administration, cannot swallow or follow instructions. Do not administer in acid or alkali poisoning. Avoid alcohol, kerosene, gasoline, metal poisoning because charcoal will not bind. No permission from medical direction. Patient already met maximum dose.
Side effects: Black stool, nausea /vomiting.
For additional treatment options go to Poisoning protocol.
Potential for seizures. Especially with DT withdrawals. Go to Seizure protocol.
Transport.
Perform ongoing assessment every 5 minutes.
Acute Abdominal Pain
Acute Abdominal Pain Signs and symptoms: Nausea / vomiting, diarrhea, cramping, vomiting blood, tachycardia (bleeding), rebound tenderness (spillage). Any complaint in the abdominal area should be evaluated by a doctor.
Evaluate responsive, airway, breathing, circulation.
If pulseless and apneic go to AED protocol and/or CPR Chart protocol.
If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
If bleed go to Hemorrhage and Shock protocol.
If OB/GYN go to Pre-delivery protocol.
Patient positioning.
- If conscious and alert place in POC, usually with knees flexed.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
Evaluate for shock internal bleeding. Go to Bleeding / Shock protocol.
PASG may be indicated for abdominal and pelvis bleeding to provide direct pressure and shock. Go to Bleeding / Shock protocol
Do not delay transport to diagnose abdominal complaints. Too difficult and not very accurate in EMS.
Reassess every 5 minutes.
Avoid narcotic pain medication until diagnosed or medical control permission.
- Kidney Stone – flank pain to groin, blood in urine.
- Gallbladder – RUQ radiating to right shoulder. 5 “f”-er
- Liver – URQ dull pain with fever, night sweats.
- Peptic Ulser – May feel better after diluting acid.
- Pancreatitis – May not feel better after eating.
- Appendicitis – RLQ to navel.
- Diverticulitis – LLQ pain and distention.
Submersion and Drowning
Submersion/Drowning
Safety first. If not trained, or do not have correct equipment (personal floatation devise – PFD) or cannot make the scene safe do not enter water. How to get out of water: Reach, throw, row and final go if you have the safety equipment and training.
Establish and maintain in-line spinal.
If not breathing, begin positive pressure ventilations with pocket mask in the water if possible.
Float backboard under patient and move to shore if possible.
More thoroughly Evaluate responsive, airway, breathing, circulation once on land. IF HYPOTHERMIC A PULSE CHECK SHOULD LAST 30 TO 60 SECONDS BEFORE STARTING CPR.
- If pulseless and apneic go to Monitor/AED protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If hypothermic go to Hypothermia protocol.
- If head or spinal injury go to Spinal Injury/Head Injury protocols.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place supine.
Always transport submersion patients.
Pre-OB
Pre-Delivery Obstetric Emergency Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- IV
- Fetal Heart Rate
- Fundus measurement (can be palpated starting at 12 weeks just above pubic bone)
Evaluate responsive, airway, breathing, circulation
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
Patient positioning
- If conscious and alert place in POC. Possibly knees flexed if abdominal pain present.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place on left side.
- Most practical deliver position: Supine with knees drawn up to chest.
If patient is pregnant, check for crowning or abnormal presenting part
- If crowning go to Active Labor and Delivery protocol. If abnormal continue with this protocol.
If an abnormal presenting part is found, such as a prolapsed cord, hand, or foot, perform the following: Position patient in knee-chest position or elevate buttocks using pillows.Nuchal Cord If both feet or butt, prepare for deliver. Watch: Breech Delivery Video
- Head will be the main concern. Ensure the cord is not pinched off by the head. Place a gloved hand in the vagina and push the head away from the cord. This also allows for an air space for baby. If head does not deliver in 3 to 5 minutes transport and call medical control.
- “From the book” Transport immediately upon recognition of any complications of a breech delivery. Administer oxygen to the mother, and keep the mother in a supine head down position with her pelvis elevated so gravity will discourage the movement of the fetus into the vaginal. If delivery cannot be slowed contact medical control for assistance to deliver or continue to transport.
If umbilical cord is prolapsed
- Insert gloved hand into vagina and push presenting part of fetus away from cord. Cover presenting part with sterile mist dressing. Rapid transport patient and notify receiving facility of situation.Knee chest position
If vaginal bleeding is present (abortion less than 20 weeks),
- First or second trimester place a sanitary napkin over vaginal opening.
- Any female with abdominal pain especially in low quadrants must role out tubal pregnancy if occurring in first trimester.
- Do not insert anything into or pack the vagina. Save tissue, save underwear. Provide emotional support and transport.
Go to Active Labor and Delivery protocol, if birth is imminent. Once fetus is delivered go to Newborn Infant protocol Transport.
- If delivery is imminent pull over and deliver unless medical control advises otherwise.
Perform ongoing assessment every 5 if unstable and 15 if stable.
No need to ever in EMS do a pelvis internal exam on a female.
Active Labor and Delivery
Active Normal Labor and Delivery Drugs that might be useful:
- Terbutaline 0.25mg to delay contractions.
- Oxytocin 10 units IV to control post fetus/placenta delivery bleeding.
Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Apply ECG
- Apply SpO2
- Apply ETCO2
- Test glucose
- IV
- Fetal Heart Rate
- Fundus measurement (can be palpated starting at 12 weeks just above pubic bone)
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If abnormal fetus presentation go to Pre-Delivery OB protocol.
Patient positioning.
- If conscious and alert place in POC. Possibly knees flexed if abdominal pain present.
- If unresponsive or confused and no trauma place in recovery position.
- If low BP place on left side.
- Most practical deliver position: Supine with knees drawn up to chest.
Delivery imminent.
- Place patient supine with knees drawn up and check for crowning.
If crowning, contractions are 2 minutes apart, duration is 45 to 60 seconds long, urge to push, prepare for delivery Check for abnormal presenting part go to Pre-OB protocol. Prepare OB kit and create sterile field. If amniotic sac still intact, rupture and remove from fetus’ face. Head delivered look for cord. Slip over head and if not possible clamp in 2 places and cut.
- Watch: Nuchal Cord Video
Suction mouth then nose of infant Continue with delivery until expelled Keep infant level with mother Go to Newborn Infant protocol Clamp the cord in 2 places (6 inches from baby then 2 more) then cut cord) Deliver placenta. If greater than 10 minutes begin to transport.
- Watch: Placenta Delivery Video
Postpartum bleeding after delivery. Watch PPH Video
- Place a sanitary napkin over vagina after placenta is delivered.
- If still bleeding place baby on mothers breast and suckle.
- If still bleeding perform uterine messages on abdomen.
- Paramedic:
❖ 10 to 20 U of Oxytocin, IM or Piggyback.
❖ IV x2 for blood loss.
Ongoing assessment 5 unstable or 15 minutes if stable
Newborn Infant
Newborn Infant Standard Care/Monitoring:
- Administer oxygen per General Difficulty Breathing Protocol
- Apply SpO2
- Test glucose (heal stick)
- APGAR score
- Provide warmth
- If you suspect generalized cold emergency go to Hypothermia protocol.
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
If meconium is present, aggressively suction airway until clear. Use suction machine if available not bulb syringe. Try to avoid over stimulation of baby to breathe until meconium removed.
Dry newborn with towels. Wrap newborn in warm towels or blanket. Be sure to cover head. Position newborn on back or lateral recumbent if large amount of secretions. Stimulate newborn by rubbing its back or flicking soles if breathing if activity is inadequate. Perform APGAR score at 1 and 5 minutes. If breathing is inadequate perform positive pressure ventilation with O2 for 30 to 60 seconds. Assess pulse.
- If heart rate is over 100 a minute assess color.
- If heart rate less than 100 but greater than 60 give 40 to 50 ventilations per minute for 30 to 60 seconds.
- If heart rate still less than 100 continue BVM until rate exceed 100 a minute.
- If heart rate is less than 60 begin CPR.
❖ Refer to CPR Chart Protocol.
Continue to reassess every 5 minutes even if stable. Support ABC, suction, dry, warm as needed. Newborns can deteriorate rapidly. Transport AHA PALS InvertedNote: Remember inverted pyramid:
- Warm dry suction, stimulate
- Basic oxygen delivery
- Aggressive oxygen delivery
- CPR
- Medications
Note: Ventilations and respirations of infant:
- Normal fluctuation is from 25 to 50 breaths per minute (can visit 60 a minute momentarily). If staying around 25 a minute stimulate. If they are staying at 60 or above provide override respiratory support and BVM to slow down rate to 40 to 50 breaths per minute.
- Grunting, see saw, or bobbing of head represents Respiratory failure. BVM them.
Note: Only use newborn equipment on newborns. Note: BVM should not have a working pop-off valve.
CPR Chart
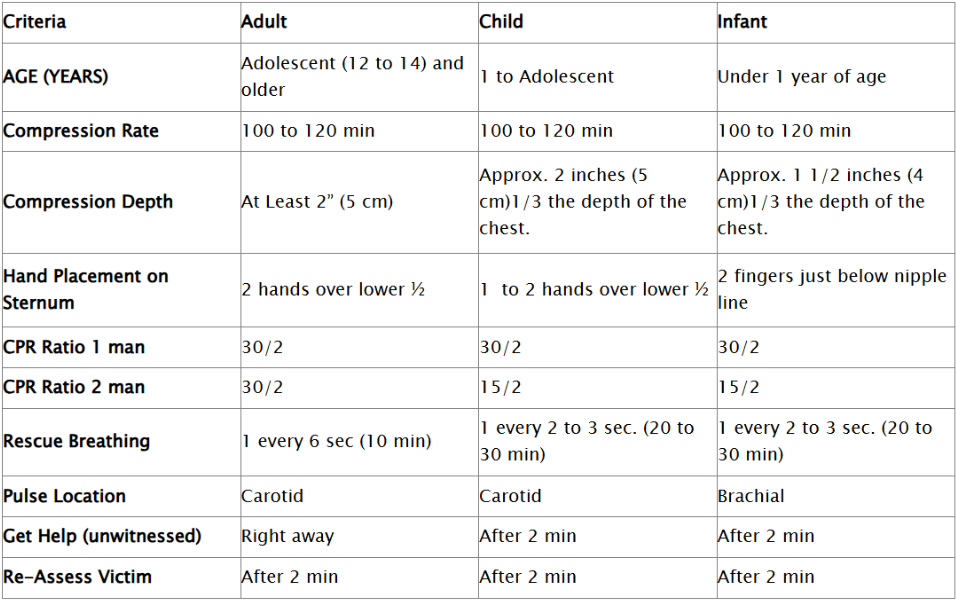
- If advanced airway (intubated, LMA, CombiTube) is placed do not have to synchronize compressions and ventilations.
- Conscious Chocking for over 1 year of age, do just like adult – abdominal thrust in and up motion from behind.
- Conscious Chocking less than 1 year of age – deliver 5 back blows (back slaps new term) and 5 chest thrust.
- Unconscious Choking over 1 year of age – treat like a cardiac arrest but just prior to ventilations look for obstruction.
- Unconscious Choking less than 1 year of age – treat like a cardiac arrest but just prior to ventilations look for obstruction.
- Never sweep an unconscious adult, child or infant for an object if you cannot see it.
- AHA Chain of Survival for adults – early help, early CPR, early defibrillation, early advanced care.
- AHA Chain of Survival for pediatrics – prevention, CPR, help, advanced care.
REVIEW THE CARDIAC MONITOR AND AED PROTOCOL.
Pediatric Respiratory Emergencies
Respiratory Emergency in the Infant or Child
Establish and maintain airway in sniffing position. If you find a child unresponsive just like an adult always open the airway with spinal precautions.
If complete foreign body airway obstruction suspected perform the following:
- Infant – head down, 5 back slaps then 5 chest thrust (or vise versa). Assess mouth finger sweep if object seen. Repeat if needed. After two sets transport and continue enroute.
- Child – Deliver 5 abdominal thrusts. Repeat twice if needed. After total of 10 abdominal thrust transport and continue enroute.
- Remember you get two sets then load and go and do more enroute.
If productive cough/cry partial obstruction place on oxygen and monitor for ineffective cough then do choking skills.
If respiratory failure, arrest, or inadequate breathing provide positive pressure ventilations at a minimum of 20 per minute if partial obstruction.
NO HUMAN (EVEN A NEWBORN) SHOULD BE BREATHING AT 60 A MINUTE OR MORE. OVERRIDE BVM AND SLOW DOWN. See General Difficulty Breathing protocol.
BLS should consider meeting up with ALS.
Expedite transport. Always try to keep the child and parent together in arms reach. Place parent on stretcher with child on lap, if possible, and safety belt both onto stretcher with own seatbelts.
If you suspect epiglottitis in a 3 year old to 7 year old do not try to visualize the oral cavity.
If you suspect croup in a 3 month to 3 year old you should hear stridor. High pitched sound heard in inhalation.
POC protect airway and humidify oxygen delivery.
Croup:
- Racemic Epinephrine 0.5mL of 2.25% nebulizer.
- 0.6mg/kg Dexamethasone IV up to 10mg in pedi patient.
Epiglottitis:
- Do not attempt intubation in field unless acute airway obstruction is present.
- If unable to intubate then cricothyroidotomy is next line of treatment.
Perform ongoing every 5 minutes stable or unstable in pediatrics
Soft Tissue Injuries
Soft Tissue Injury
Maintain manual c-spine support if head and neck injury suspected or unknown
Evaluate responsive, airway, breathing, circulation
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If bleeding or shock go to Bleeding and Shock protocol.
Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
Control any major life-threatening bleeding
- Non-Multisystem trauma:
❖ Direct pressure, elevate, pressure point (femoral or brachial only), tourniquet (last resort).
- Multisystem trauma:
❖ Direct pressure then move to tourniquet.
Maintain body temperature and keep patient calm
If open chest injury (sucking chest wound)
- Apply non-porous dressing. Secure on three sides and make a flutter dressing. Or secure of all four side. For testing purposes if you have to pick between taping 3 or 4 sides always pick 3 sides.
- Airway priority. Once securing the airway and ensure adequate ventilations, place a gloved hand over the chest wound until an occlusive dressing can be applied.
- If respirations deteriorate after placing occlusive dressing, unseal while patient exhales.
- Paramedic Care:
❖ Needle decompression
➤ 2 and 3 intercostal space midclavicular
➤ 5 and 6 intercostal space midaxillary
❖ If suspected hemo do not decompress. If hemo is tapped close needle.
If abdominal bleed with tenderness and/or pelvic pain
- Consider PASG. See Bleeding and Shock protocol for indications and contraindications.
➤ PASG can provide direct pressure.
If evisceration
- Apply moist sterile dressing and flex knees if possible.
- Do not contaminate.
- Do not replace organs.
If large neck laceration
- Control bleeding and apply a non-porous dressing.
- While securing airway place a gloved hand over the neck wound.
If impaled object
- Apply dressing to wound and then stabilize the impaled item in place.
- Remove only if impaled in cheek and obstructing airway. Removing object in same direction it entered. Reverse the path.
If avulsion
- Partial – Rinse wound to clean off debris if necessary.
- Partial – Apply dressing and bandage to keep avulsed tissue in place.
- Complete – treat as amputated part.
If amputation (partial)
- Realign extremity to as normal as possible.
If amputation (complete)
- Control bleeding and treat patient first.
- Wrap part in sterile dressing place in bag and place in cool place.
If bitten by vector borne (animal) or humans
- Should always be advised to seek medical attention.
- Perform emergency move if scene is not safe to EMS and patient.
- Wash the wound with soap and water.
- Dress with a dry dressing.
Transport. Golden hour 10 minute on scene time
Ongoing assessment 5 unstable or 15 stable
Pain management, as needed
- Morphine 2-4mg IV max 10mg.
- Fentanyl 50 – 200 mcg IV or IN.
Burn Injuries
Burn Emergency
Remove patient from burning source and stop burning if safe to do so.
- Stop/drop/roll, smother, water….
- Remember infection kills. EMS should wear entire PPE available.
Maintain manual c-spine support if head and neck injury suspected or unknown
Evaluate responsive, airway, breathing, circulation. ECG, IV’s, Blood Sugar
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General SOB protocol to maintain airway if needed then return to this protocol.
- Aggressive airway management of evidence of inhalation injury.
- If bleeding or shock go to Bleeding and Shock protocol.
Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
Estimate severity of burn
- Body surface area (BSA) using rules of 9.
- Estimate depth of burns.
- Priority burns: Less than 5 years of age and over 55 years of age. Burns to feet, hands, groin, chest, face. Inhalation burns, and circumferential burns.
Apply sterile dressing and bandage or burn sheet
- Keep loose because of swelling.
If BSA less than 10% dress wet.
- Dress all other burns dry. When in doubt keep dry.
Maintain body temperature
If IV emergency fluid resuscitation is needed to maintain perfusion.
- Parkland Burn Formula
- 4mL/kg of body weight times % BSA burned (2nd &3rd degree only) will be the fluid given during the first 24 hours. (formula is: 4X weight X Burned %).
- Give half of this amount during the first 8 hours from the time of injury.
- Lactated Ringers is the preferred fluid.
Pain Management
- Morphine 2-4mg IV max 10mg.
- Fentanyl 50 – 200mcg IV or IN.
Manage other associated injuries
Dry chemical burn
- Brush off and remove clothing and flush for 20 minutes.
Liquid chemical burn
- Remove clothing flush 20 minutes.
Chemical burn to eyes
- Flush 20 minutes
- Open eye lids unless fused closed and flush.
Thermal burns to eyes
- Do not open eyelids.
- Apply moist sterile dressing to both eyes.
Electrical burns
- If cardiac arrest suspect V-fib.
- Apply ECG monitor.
- Monitor pulse and respirations.
- Look for entrance and exit wounds.
- Look for pathway (entrance and exit wounds). Foot to foot, foot to arm, arm to arm most common.
Ongoing assessment 5 unstable and 15 stable
Musculoskeletal Injuries
Musculoskeletal Injury
Maintain manual c-spine support if head and neck injury suspected or unknown
- Evaluate responsive, airway, breathing, circulation
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If bleeding or shock go to Bleeding and Shock protocol.
Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
Dress/bandage all open wounds prior to splinting
If fracture is grossly deformed or no distal pulse
- Apply gentile traction and attempt to realign.
- If excruciating pain or resistance is met, stop and splint in the position found.
Splint suspected dislocations and knee
- Splint in position found unless no pulse present.
Hip dislocation or fracture
- Pad between both legs and bind together.
- Or apply long board splints and place on back board.
- Or pelvis apply PASG inflate all three sections to splinting pressure.
- Or pad between legs and bind legs together and place on back board.
Femur Fracture
- Must be isolated mid-shaft femur fracture for traction splint.
- If using PASG with traction splint, the PASG goes on first then traction over PASG.
- Apply traction splint and then back board to move.
Upper extremity injury
- Shoulder sling and swathe.
- Move arm to normal position if possible.
- Place hand in position of function if possible.
Always reassess PMS and document
Transport
Ongoing assessment 5 unstable and 15 stable
Pain management, as needed
- Morphine 2-4mg IV max 10mg.
- Fentanyl 50-200mcg IV or IN
Eye Injuries
Eye Injury
Maintain manual c-spine support if head and neck injury suspected or unknown
Evaluate responsive, airway, breathing, circulation
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If bleeding or shock go to Bleeding and Shock protocol.
Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
Foreign object in eye
- If possible transport patient for further evaluation and removal of the object by emergency department staff.
- Only attempt to remove non-embedded objects on the conjunctiva.
- Do not attempt remove of objects on or lodged in the cornea.
- No not administer anesthetic drops if outer layers have been ruptured.
- To remove a foreign object from the conjunctiva flush with water.
- If not successful and under the upper lid, draw upper lid down over lower lid.
- If object remains lift lid with cotton swab and remove with corner of sterile gauze or swab.
Orbital injury if eyeball not injured
- Place ice packs over injured eye.
- If eyeball injured do not use cold packs.
- Refer to Globe injury below.
Lid injury control bleeding
- With light pressure control bleeding.
- Do not use pressure if eyeball is injured also.
- Cover lid with sterile gauze in saline.
- No not administer anesthetic drops.
Preserve avulsed skin and transport with patient if needed
- No not administer anesthetic drops.
If eyeball injury is not suspected
- Cover lid with cold compress, patch both eyes.
- If irritation administer anesthetic Tetracaine 1-2 drops ever 15 minutes as needed.
❖ Due to preservatives in Tetracaine eye may burn for a few seconds prior to numbing effects.
Injury to the globe
- Apply patches to both eyes.
- Do not apply pressure.
- Apply a eye shield to injured eye.
- Keep patient supine.
- No not administer anesthetic drops.
Chemical burn to eye
- Irrigation with water for 20 minutes.
- Do not contaminate uninjured eye.
- Force lids open if needed to flush.
- If irritation (example mace) administer anesthetic Tetracaine 1-2 drops ever 15 minutes as needed.
Remove contact lenses
- If not going to aggravate the wound remove contacts.
Transport
Ongoing every 5 unstable and 15 stable
Head Injury
Head Injury
Signs/Symptoms: Hallmark sign is altered mental status.
- Maintain manual c-spine support if head and neck injury suspected or unknown.
- Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty protocol to maintain airway if needed then return to this protocol.
- If bleeding or shock go to Bleeding / Shock protocol.
Patient positioning.
- If trauma place on backboard.
- If low BP or unresponsive place supine and elevate legs.
- If BP normal/to high elevate head 15 degrees.
When controlling bleeding be careful not to apply excessive pressure to a open skull fracture.
Elevate head 8 to 10 inches if BP is acceptable.
Transport. Golden hour 10 minutes on scene.
Be prepared for Cushing’s: Slow pulse, high BP, erratic respirations, projectile vomiting, widening pulse pressure.
Be prepared for seizures. Go to Seizure protocol.
Ongoing every 5 unstable and 15 sable.
Avoid Nitro, Glucose.
Helmet removal:
- If good fit, no need to assess head, and can immobilize in a neutral position leave helmet on.
- If not good fit, you need to do airway skills, or cannot immobilize in a neutral position remove helmet.
Note: If patient meets the criteria to BVM in the General SOB protocol consider hyperventilating the head injured victim at about 24 breaths per minute (35 to 40 torr ETCO2) to blow off CO2. If posturing is present ventilate to 30 to 35 torr ETCO2.
Spine Injury
Spinal Injury
Signs/Symptoms: Best signs are paralyzed, numbness in extremities.
Maintain manual c-spine support if head and neck injury suspected or unknown.
Evaluate responsive, airway, breathing, circulation.
If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
If bleeding or shock go to Bleeding / Shock protocol.
Patient positioning.
- If trauma place on backboard.
- If low BP place supine.
Immobilization devise.
- Place on long board if unstable. Use a minimum of 3 straps. Secure torso then head.
- Place in short board (KED) if stable and found in seated position. Secure torso then head then place patient on long board for transport.
- If you find them walking at the scene stop movement immediately and long board in a standing position.
- Note: When placing a cervical collar evaluate the neck prior to covering. Advise conscious patient it is going to be unconfortable.
- Check PMS prior to placement and throughout transport for changes.
Shock.
- If BP and heart rate slow or regular, skin pale and cool, and clammy think neurogenic shock. Go to Bleeding / Shock protocol.
- If BP low and heart rate fast suspect hypovolemic shock. Go to Bleeding / Shock protocol.
- Transport. Golden hour 10 minutes on scene.
- Ongoing every 5 minutes if unstable and every 15 minutes if stable.
Note: Spinal immobilization is required for the following:
- Significant MOI who have an altered LOC, intoxicated, complain of head-neck-back pain.
- Significant trauma above the nipple line.
- Symptoms of neurological injuries.
- Tenderness to neck-spine with palpation.
- Penetrating injury: Strong suspicion of spinal injury based on location of injury.
Chest Injury
Chest Injury
Maintain manual c-spine support if head and neck injury suspected or unknown.
Evaluate responsive, airway, breathing, circulation.
If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
If bleeding or shock go to Bleeding / Shock protocol.
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
If obvious open chest wound.
- Place glove hand over wound until non-porous material dressing is used.
- If open chest wound is occluded with a dressing and patient suddenly begins to deteriorate, lift dressing off wound during exhalation to relieve trapped air then reapply dressing. Also see Soft issue Injury protocol.
Impaled object stabilize in place after controlling bleeding.
Flailed segments/ non-intact chest wall.
If inadequate breathing begin positive pressure ventilation. If available BVM may have limited use. If Positive Flow Ventilator (40+ LPM) is available use it.
Place glove hand over broken segment then stabilize with blanket, pillow, bulky dressing.
Do not use sand bags / IV bags to splint flailed segments.
Transport.
Ongoing every 5 minutes if unstable and every 15 minutes if stable.
Facial Injury
Facial Injury
Maintain manual c-spine support if head and neck injury suspected or unknown.
Evaluate responsive, airway, breathing, circulation.
- If pulseless and apneic go to AED protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If bleeding or shock go to Bleeding / Shock protocol
Patient positioning.
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
- Be careful not to apply excessive pressure to an open skull fracture.
- Apply a moist dressing to any exposed tendons, ligaments, or exposed bones.
- Avulsed tooth.
Place in cup of sterile water or wrap in gauze soaked in saline.
Control bleeding from tooth socket with gauze pad.
Make sure the gauze pad does not become a choking hazard.
Optional storage of tooth: treat just like an amputated part in a cool place.
- Foreign object in cheek that did not penetrate completely through the cheek use bulky dressing to stabilize.
- Foreign object penetrated through to other side.
Remove in same direction it entered if interfering with airway control. Reverse the path.
Pack dressing between gums and cheek to control bleeding.
Injury to nose (Epistaxis).
- Lean forward, pinch, ice and spit out blood.
- Check BP in elderly patient, might be high.
- If patient has clotting problems transport immediately.
Injury to ear.
- Save avulsed parts.
- Do not probe or pack the ear.
- Place loose dressing to absorbed blood and fluid.
- No pressure.
- Do not try to remove an object in the ear.
Bleeding from ear or nose with head injury.
- Do not pack.
- Place loose dressing to absorb blood.
- Perform target (halo) test. If positive go to Head Injury protocol.
Transport.
Ongoing every 5 minutes if unstable and every 15 minutes if stable.
Bleeding and Shock
Bleeding and Shock
Evaluate responsive, airway, breathing, circulation
- If pulseless and apneic go to AED/Cardiac Monitor protocol and/or CPR Chart Protocol.
- If breathing difficulty if present go to General Difficulty Breathing protocol to maintain airway if needed then return to this protocol.
- If impaled object go to Soft Tissue Protocol
- If evisceration go to Soft Tissue Protocol
- If avulsion go to Soft Tissue Protocol
- If amputation go to Soft Tissue Protocol
Standard Care/Monitoring:
- Administer oxygen high flow.
- ECG
- SpO2
- ETCO2
- Establish 2 IV’s
- Keep patient warm.
- Minimize patient exertion.
Maintain manual c-spine support if head and neck injury suspected or unknown Evaluate responsive, airway, breathing, circulation Patient positioning
- If conscious and alert place in POC.
- If unresponsive or confused and no trauma place in recovery position.
- If trauma place on backboard.
- If low BP place supine.
Control any major life-threatening bleeding that is multitrauma or severe bleeding. If direct pressure cannot maintain control go straight to tourniquet Isolated mild/moderate bleeding without multisystem trauma: Direct pressure, elevate, pressure point (femoral or brachial only), tourniquet (last resort) Maintain body temperature and keep patient calm If abdominal tenderness and pelvic pain indicating internal bleeding or large soft tissue injuries of lower extremities consider PASG for direct pressure and splinting.
- PASG contraindicated entirely for CHF / Pulmonary Edema patient.
- SEPTIC is when correct to use legs but not abdomen section. Systolic over 100mmHg, Evisceration, Pregnant in 2/3 trimester, Thumper used for CPR, Impaled object, Chest trauma that needs free movement of diaphragm.
- Note: If used for shock pump to 90mmHg. If used to control bleeding inflate for direct pressure but so not to interfere with PMS.
- NOTE: For lower leg fractures and bleeding (tibia and fibula) use the PASG if available. It will provide direct pressure and stabilize the region. Do not worry about bone ends popping the PASG if used for lower leg bleeding.
- Note: Inflate or deflate PASG only with medical control permission.
If shock, keep patient calm, give oxygen, keep warm, and elevate the feet Fluid replacement
- Low-resistance shock (anaphylaxis, septic, neurogenic) infuse 250mL IV boluses as needed to a max of 1 liter.
- Uncontrolled bleeding with shock deliver enough fluid to maintain a radial pulse (80-90mmHg).
- Pediatric: 20mL/Kg IV fluid x 3.
- Adult: Consult medical control once 500mL IV boluses start to total 20mL/kg. At this point fluid may bee diluting blood too much.
Cardiogenic shock
- BP of 70 to 90mmHg Dopamine 2-20mcg/kg/min.
- BP less than 70mmHg Levophed drip at 0.5-12mcg/min.
Ongoing every 5 minutes Transport
- Golden hour 10 minute on scene time. LOAD AND GO!
Patient Refusal
Patient Refusal of Treatment or Transport click here to view “refusal form”.
- Once a duty to act is present the goal of EMS is to transport the patient to the hospital.
- If patient asks EMS for advise if transport is necessary the response is, “we are unable to determine the need at this time.”
- EMS will follow patients request for transport even if transport is unnecessary.
Refusal Requirements
- Patient must initiate the refusal.
- Age of 18 years old or older (May be less depending on medical director and state).
❖ Exception
➤ Emancipated Minor Exception
➤ Legally Married Exception
➤ Pregnant Exception
➤ Active Military Service
- Patient must be A&Ox4
- Patient judgment not influenced by alcohol or drugs (prescription or recreational) use.
- Patient must have control of basic body functions. (stance, balance)
- Patient has no imminent feelings, plan or means of suicide.
- Patient vital signs within normal limits.
- Patient has no evidence of life or limb threatening injury or illness.
Granting Refusal
- A minimum of two on scene EMS professionals must agree.
- If above criteria is clearly met a refusal may be granted.
- If above criteria is questionable contact medical control.
Documentation of Refusal
- Complete standard patient evaluation forms.
- Document A&Ox4.
- Document that transport was offered and refused.
- Document age of patient.
- Document that a witness observed the situation. Obtain signature of witness. (Bystander, Family Member)
- Document that above criteria was met in full.
- Document signature of at least two on scene EMS professionals.
- Document that the statement was made that by EMS granting this refusal doe not suggest that there is no need to be seen by a doctor.
- Document the signature of patient. (A minor may not sign only the agent – parent, adopted parent, legal guardian, law enforcement).
Care Options
- Patient may consent to treatment but not transport.
- Patient may consent to transport but not treatment.
- At any time the patient may terminate consent if above criteria is met for granting refusal.
Family Violence
Family Violence
- Treat injuries and illness as necessary.
- Document observations and care provided.
- Must give the patient/victim referral information for family notice.
❖ Local police number
❖ Local shelters or social organizations and phone numbers.
❖ Advice the victim to seek legal aid.
❖ Provide notice in commonly used language of victim.
Info to be given to patient: Click here for: “Family Violence Form – English“. Also comes in Spanish.
Child Abuse and Elderly Abuse
Child and Elderly Abuse
Consider law enforcement to gain entry if scene becomes physically unstable or dangerous to abused patient or EMS.
If family members are allowing EMS to treat abuse patient and you suspect abuse advise receiving facility of your suspicions because a doctor is specifically trained to identify abuse.
Do not ask to recreate the situation or answer questions while still in the abusive environment.
Have a trained profession in abuse interview the patient. Not EMS.
Your main goal is assessment and treatment.
Do not questions the care givers about the abuse.
Do not let the abused patient be left alone with the abuser.
Provide accurate and objective documentation.
Do not allow abuser(s) to know EMS suspects abuse. Keep mouth shut. Do not show your cards to abuser!
Dead Upon Arrival and DNR
Dead upon Arrival
- Obvious expiration; rigor mortis, livor mortis (lividity), decapitation, visible brain matter, decomposition.
- Note: Warmth is not a determining factor.
- Multiple Casualty Incident – If pulseless at time of assessment – receive a black tag. If arrest after assessment receive a red tag.
- Preserve chain of evidence. Do not disturb the scene. Document anything your touch and move.
Do Not Resuscitate
- The form can be an original or exact copy.
- Must be the Texas-Out-of-Hospital DNR Form
❖ Click here for: Tx DNR Form
- Upon determining a valid DNR order the following are withheld or withdrawn;
❖ CPR
❖ Artificial Ventilation
❖ AED
- A “qualifying person” may override the DNR. (listed on back of DNR)
- If cardiac arrest is result of a crime or if pregnant the DNR does not apply.
- Contact medical control for assistance.
DO NOT DELAY CARE TO VALIDATE THE DNR. AS RESPONDERS ARRIVE AND RESOURCES PERMIT THEN VALIDATE THE DNR.
Pending Protocols
Collapse content goes here….
ACLS
V-Fib / Pulseless V-Tach
Ventricular Fibrillation & Pulseless Ventricular Tachycardia
Primary Assessment
Airway (basic) – Breathing – Circulation (CPR) If down time is longer than 4 minutes perform 2 minutes of CPR prior to electrical therapy.
Defibrillate at 360J (or equivalent Biphasic energy) followed by 2 minutes of immediate CPR
_______________________________________________________
Secondary Assessment Airway (advanced) Breathing (confirm by at least 2 methods) Circulation (IV/IO access x 2) Differential (search for and treat causes)
________________________________________________________
Vasopressors Epinephrine 1mg every 3-5 minutes. or Vasopressin 40 U IV bolus given once. May replace 1st or 2nd dose of EPI.
________________________________________________________
Antiarrhythmics Amiodarone – 300mg IV bolus diluted in 20-30mL of NS. Consider repeat dose of 150mg in 3-5 minutes. If defibrillation successful start 1mg/min infusion for 6 hours.
If Amiodarone is not available Lidocaine – 1.5mg/kg bolus. Repeat at 1.5mg/kg 3-5 minutes after first dose. If defibrillation successful start 1-4mg/min infusion. or Magnesium – 1-2g IV diluted in 10mL of D5W if Torsades de Pointes or hypomagnesemia.
________________________________________________________
Sodium Bicarbonate – 1mEq/kg may repeat in 10 minutes at 0.5mEq/kg. Given if known metabolic acidosis.
_______________________________________________________
Note: ETT drugs – double dose in 10mL. Note: Epinephrine is given on its own time schedule.
Asystole
Asystole
Primary Assessment Airway (basic) – Breathing – Circulation (CPR)
___________________________________________________
Secondary Assessment Airway (advanced) Breathing (confirm by at least 2 methods) Circulation (IV/IO access) Differential (search for and treat causes) PATCH-5-MD
______________________________________________________
Epinephrine 1mg every 3-5 minutes or Vasopressin 40 U IV bolus given once. May replace 1st or 2nd dose of EPI.
__________________________________________________
Consider Sodium Bicarbonate 1mEq/kg may repeat in 10 minutes at .5mEq/kg. Known hyperkalemia, Cyclic antidepressant overdose, or long down time.
__________________________________________________
Consider termination of efforts
_________________________________________________
Note: ETT drugs – double dose in 10mL. Note: Epinephrine is given on its own time schedule. Note: EPI per 2005 guideline is not preferred via ETT.
Causes:
- P pulmonary embolism
- A acidosis
- T tension pneumo
- C cardiac tamponade asystole
- H hypovolemia
- H hypoxia
- H heat/cold
- H hyper/hypokalemia
- H hypoglycemia
- M MI
- D drug overdose
PEA
Pulseless Electrical Activity
Primary Assessment Airway (basic) – Breathing – Circulation (CPR)
_________________________________________________________
Secondary Assessment Airway (advanced) Breathing (confirm by at least 2 methods) Circulation (IV/IO access) Differential (search for and treat causes) PATCH-5-MD
__________________________________________________________
Epinephrine 1mg every 3-5 minutes or Vasopressin 40 U IV bolus given once. May replace 1st or 2nd dose of EPI.
___________________________________________________________
Consider Sodium Bicarbonate 1mEq/kg may repeat in 10 minutes at .5mEq/kg. Known hyperkalemia, Cyclic antidepressant overdose, or long down time
__________________________________________________________
Consider termination of efforts
___________________________________________________________
Note: PEA is any pulseless rhythm other than asystole, V-tach, or V-Fib
Causes:
- P pulmonary embolism
- A acidosis
- T tension pneumo
- C cardiac tamponade asystole
- H hypovolemia
- H hypoxia
- H heat/cold
- H hyper/hypokalemia
- H hypoglycemia
- M MI
- D drug overdose
Bradycardia
Bradycardia
Primary Assessment Airway (basic) – Breathing – Circulation
______________________________________________________
Secondary Assessment Airway (advanced) Breathing (confirm by at least 2 methods) Circulation (IV access) Differential (search for and treat causes)
_____________________________________________________
Determine if STABLE or UNSTABLE If stable continue work-up. If unstable continue with algorithm.
____________________________________________________
Narrow QRS Bradycardia, Sinus Brady, Junctional Rhythm, 2 Degree AV Block, type 1 TCP as soon as possible Atropine 0.5mg IV every 3-5 minutes to max dose of 0.04mg/kg or 3mg
Complete AV Block, Wide QRS Bradycardia, 2 Degree AV Block, type 2, Complete AV Block, Idioventricular Rhythm Pacing is preferred treatment
_________________________________________________
If BP still slow after treating rate consider:
Dopamine 5-20mcg/kg/min and/or Epinephrine Drip – 2-10mcg/min then Isoproterenol Drip – 2-10mcg/min
STV (Narrow Complex Tachycardia
Narrow Complex Tachycardia
Primary Assessment Airway (basic) – Breathing – Circulation
_______________________________________________
Secondary Assessment Airway (advanced) Breathing (confirm by at least 2 methods) Circulation (IV access) Differential (search for and treat causes)
__________________________________________________
If Stable continue with algorithm. If Unstable go to bottom box and deliver electrical therapy.
__________________________________________________
Attempt therapeutic diagnostic maneuver Vagal stimulation Adenosine 6mg rapid push IV, may repeat in 1-2 minutes at 12mg.
_________________________________________________
Refractory to Adenosine B-Blocker Ca2+ channel blocker
__________________________________________________
If hemodynamically unstable, synchronize cardioversion at 100J, 200J, 300J, 360J (or equivalent Biphasic energy). Remember to check for a pulse after each shock.
V-Tach with a Pulse
Ventricular Tachycardia: Monomorphic and Polymorphic
Primary Assessment Airway (basic) – Breathing – Circulation
______________________________________________________
Secondary Assessment Airway (advanced) Breathing (confirm by at least 2 methods) Circulation (IV access) Differential (search for and treat causes)
______________________________________________________
If Stable continue with algorithm. If Unstable go to bottom box and provide electrical therapy. Note!!!!! May go directly to cardioversion
_________________________________________________________
Stable Polymorphic V-tach Is QT baseline interval prolonged?
Magnesium 1 to 2g in 20mL D5W
Amiodarone 150 mg IV bolus over 10 minutes or Lidocaine 0.5 to 1mg/kg IV push
Synchronized cardioversion
__________________________________________________________
Stable Monomorphic V-tach
Amiodarone 150 mg IV bolus over 10 minutes or Lidocaine 0.5 to 1mg/kg IV push
Synchronized cardioversion
__________________________________________________________
If hemodynamically unstable, synchronize cardioversion at 100J, 200J, 300J, 360J (or equivalent Biphasic energy) Remember to check for a pulse after each shock.
Note: Once a patient has received electrical therapy all ventricular drugs should then be followed by another shock.
Pending Protocol
Collapse content goes here….
PALS
V-Fib and V-Tach Pulseless
Ventricular Fibrillation & Pulseless Ventricular Tachycardia
Primary Assessment Airway (basic) – Breathing – Circulation (CPR) Defibrillate (immediately) 2J/kg or equivalent Biphasic energy. Followed by immediate CPR for 2 minutes. Additional shocks are at 4J/kg.
___________________________________________
Secondary Assessment Airway (basic or advanced) Breathing (confirm by at least 2 methods) Circulation (IV/IO access) Differential (search for and treat causes)
____________________________________________
Epinephrine 0.01mg/kg IV (1:10000) or 0.1mg/kg ETT (1:1000) every 3-5 minutes
____________________________________________
Antiarrhythmics
Amiodarone – 5mg/kg IV bolus. If defibrillation successful start 5 to 10mcg/kg/min infusion. or Lidocaine – 1mg/kg bolus. Repeat at 1mg/kg 3-5 minutes after first dose. If defibrillation successful start 20 to 50mcg/kg/min infusion. or Magnesium – 25 to 50mg/kg IV if Torsades de Pointes or hypomagnesemia. or Procainamide – 15mg/kg over 30 minutes.
________________________________________________
Sodium Bicarbonate – 1mEq/kg may repeat in 10 minutes at 0.5mEq/kg. Given if known metabolic acidosis.
_______________________________________________
Note: Do not interrupt CPR for longer than 10 seconds at a time. Note: ETT drugs – double dose in 5mL. Note: Epinephrine is given on its own time schedule.
Asystole
Asystole
Primary Assessment Airway (basic) – Breathing – Circulation (CPR)
________________________________________________
Secondary Assessment Airway (basic and advanced) Breathing (confirm by at least 2 methods) Circulation (IV/IO access) Differential (search for and treat causes) PATCH-5-MD
__________________________________________________
Epinephrine 0.01mg/kg IV (1:10000) or 0.1mg/kg ETT (1:1000) every 3-5 minutes.
__________________________________________________
Atropine – 0.02mg/kg IV every 3-5 minutes to max dose of 0.04mg/kg. Minimum single does 0.1mg maximum single dose 0.5 for child and 1mg for adolescent.
__________________________________________________
Consider Sodium Bicarbonate 1mEq/kg may repeat in 10 minutes at 0.5mEq/kg. Known hyperkalemia, Cyclic antidepressant overdose, or long down time
_________________________________________________
Consider termination of efforts
Causes:
- P pulmonary embolism
- A acidosis
- T tension pneumo
- C cardiac tamponade asystole
- H hypovolemia
- H hypoxia
- H heat/cold
- H hyper/hypokalemia
- H hypoglycemia
- M Myocardial abnormalities
- D drug overdose
PEA
Pulseless Electrical Activity
Primary Assessment Airway (basic) – Breathing – Circulation (CPR)
_________________________________________________________
Secondary Assessment Airway (basic and advanced) Breathing (confirm by at least 2 methods) Circulation (IV/IO access) Differential (search for and treat causes) PATCH-5-MD
__________________________________________________________
Epinephrine 0.01mg/kg IV (1:10000) or 0.1mg/kg ETT (1:1000) every 3-5 minutes.
_________________________________________________________
If bradycardic Atropine – 0.02mg/kg IV every 3-5 minutes to max dose of 0.04mg/kg. Minimum single does 0.1mg maximum single dose 0.5 for child and 1mg for adolescent.
If bradycardic consider TCP as soon as possible.
_______________________________________________________
Consider Sodium Bicarbonate 1mEq/kg may repeat in 10 minutes at .5mEq/kg. Known hyperkalemia, Cyclic antidepressant overdose, or long down time
_____________________________________________________
Consider termination of efforts
Note: PEA is any pulseless rhythm other than asystole, V-tach, or V-Fib
Causes:
- P pulmonary embolism
- A acidosis
- T tension pneumo
- C cardiac tamponade asystole
- H hypovolemia
- H hypoxia
- H heat/cold
- H hyper/hypokalemia
- H hypoglycemia
- M Myocardial abnormalities
- D drug overdose
Bradycardia
Bradycardia
Primary Assessment Airway (basic) – Breathing – Circulation
_____________________________________________
Secondary Assessment Airway (basic and advanced) Breathing (confirm by at least 2 methods) Circulation (IV access) Differential (search for and treat causes)
___________________________________________
Determine if STABLE or UNSTABLE If stable continue work-up. If unstable continue with algorithm.
_______________________________________________
If Severe Cardiorespiratory Compromise and heart rate less than 60 per minute start CPR.
______________________________________________
Epinephrine 0.01mg/kg IV (1:10000) or 0.1mg/kg ETT (1:1000) every 3-5 minutes.
______________________________________________
Atropine 0.02mg/kg IV every 3-5 minutes to max dose of 0.04mg/kg. Minimum single does 0.1mg maximum single dose 0.5 for child and 1mg for adolescent. TCP as soon as possible
__________________________________________
Once rate is addressed consider the following for low BP
Epinephrine Drip – .1-1ug/kg/min and/or Dopamine 2-20mcg/kg/min
Title or SVT (Narrow Complex Tachycardia)Question
Narrow Complex Tachycardia
Primary Assessment Airway (basic) – Breathing – Circulation
__________________________________________________
Secondary Assessment Airway (basic and advanced) Breathing (confirm by at least 2 methods) Circulation (IV access) Differential (search for and treat causes)
____________________________________________________
If Stable continue with algorithm. If Unstable go to bottom box and deliver electrical therapy. Infant HR >220 Child HR >180
____________________________________________________
Attempt therapeutic diagnostic maneuver Vagal stimulation
Adenosine 0.1mg/kg rapid push IV, may repeat in 1-2 minutes at 0.2mg/kg. Max dose 3 times given
_____________________________________________________
If hemodynamically unstable, synchronize cardioversion at .5-1J/kg then 2J/kg (or equivalent Biphasic energy). Remember to check for a pulse after each shock. (Some protocols may indicate 1j/kg, 2j/kg, 3j/kg and 4j/kg)
V-Tach with a Pulse
Ventricular Tachycardia
Primary Assessment Airway (basic) – Breathing – Circulation
_____________________________________________
Secondary Assessment Airway (basic and advanced) Breathing (confirm by at least 2 methods) Circulation (IV access) Differential (search for and treat causes)
________________________________________________
If Stable continue with algorithm. If Unstable go to bottom box and provide electrical therapy. Note!!!!! May go directly to cardioversion
___________________________________________________
Antiarrhythmics
Amiodarone – 5mg/kg IV bolus over 20 to 60 minutes. If defibrillation successful start 5 to 10mcg/kg/min infusion. or Lidocaine – 1mg/kg over 5 to 10 minutes. If defibrillation successful start 20 to 50mcg/kg/min infusion. or Procainamide – 15mg/kg over 30 to 60 minutes.
____________________________________________________
If hemodynamically unstable, synchronize cardioversion at 0.5-1J/kg then 2J/kg (or equivalent Biphasic energy) Remember to check for a pulse after each shock.
Note: Once a patient has received electrical therapy all ventricular drugs should then be followed by another shock.
Pending Protocol
CONTACT EMTS
Please feel free to contact us with any questions regarding our programs.
PHONE (972) 527-3687
ADDRESS
3410 Midcourt Rd
Suite 136
Carrollton, TX 75006
Contact Us
Thank you for contacting us. We'll get back to you shortly.
Feel free to also contact us in the following channels:
Phone: 972-527-3687
Email: tcellio@emts911.com
Facebook: https://facebook.com/EMTS911/
Please try again later.
